
Perceived Coercion Among Jail Diversion Participants in a Multisite Study
Individuals with serious mental illness are significantly overrepresented in the criminal justice system. Recent estimates suggest that approximately two million people with serious mental illness are booked into U.S. jails each year ( 1 ). Moreover, after this initial arrest, people with serious mental illness are more likely to be detained in jail (as opposed to being released or having their cases dismissed) and, once jailed, to stay incarcerated 2.5 to 8.0 times longer than their counterparts without mental illness ( 2 ).
To address this growing problem, jail diversion programs for people with mental illness have dramatically increased in the United States ( 3 ). These programs divert people with mental illness from jails and connect them to community-based behavioral health services with the explicit goal of decreasing future criminal justice involvement and improving mental health outcomes. Despite the popularity of jail diversion, evidence of its effectiveness is limited ( 3 , 4 , 5 , 6 ). Further, little is known regarding the extent to which participants feel coerced into diversion programs and how perceived coercion may undermine the goals of the diversion program.
Studies of perceived coercion among patients in mental health treatment suggest that although legally mandated treatment is often associated with higher levels of perceived coercion, considerable variation exists, and other factors such as respect, empathy, and choice are often more important than legal status in explaining perceived coercion ( 7 , 8 , 9 , 10 ). Findings are also mixed with regard to the association between perceived coercion and adherence to outpatient treatment or medication ( 9 , 11 , 12 , 13 ).
Unlike court-ordered (involuntary) treatment, there is no objective coercion involved in jail diversion because entering a diversion program is voluntary for participants. However, jail diversion takes place within the criminal justice system, and it is the perception of coercion (that is, lack of choice or control) in the process of receiving treatment that is most important. Therefore, it seems especially important to examine perceived coercion within the context of jail diversion and to better understand the effect that perceived coercion may have on the ability of diversion programs to engage and maintain participants in behavioral health services. This study was designed to address the following questions: What factors account for perceived coercion into entering the diversion program? What factors account for perceived coercion into receiving behavioral health services? Finally, does perceived coercion at baseline predict use of behavioral health services over the following year?
Methods
Procedures
Thirteen jail diversion programs funded from 2002 to 2004 through the Targeted Capacity Expansion Jail Diversion Initiative of the Substance Abuse and Mental Health Services Administration (SAMHSA) were included in this study. Funding provided over three years was used to develop the diversion programs and establish links across service systems to facilitate access to treatment for diverted individuals. Participants at each of the sites were eligible for diversion if they were identified in jail as having a DSM-IV axis I diagnosis. Most programs focused on persons who had committed nonviolent misdemeanors, although persons with felonies and some violent charges were allowed into some diversion programs. Data were collected from February 2003 to July 2005. Baseline interviews were conducted with 905 individuals enrolled in the postbooking jail diversion programs. Participants were interviewed by trained independent interviewers at baseline and six months and 12 months later. Data from the baseline and 12-month interviews are reported here. Informed consent was obtained from participants, and study protocols were approved by institutional review boards at each of the 13 sites.
Measures
An interview protocol required by SAMHSA for purposes of program evaluation was administered to all participants. The interview included Government Performance Reporting Act questions on demographic characteristics (gender, race and ethnicity, date of birth, education level, employment, income, and housing status) and alcohol and drug use. Questions on substance use assessed days of use in the 30 days before arrest or jail detention. The number of reported days of drinking to intoxication and using illegal drugs was used to construct a substance abuse variable with three levels: none, moderate, and heavy.
Participants were asked dichotomous (yes-no) questions regarding the experience of a range of traumatic events. The questions assessed whether participants experienced physical assault ("has anyone choked, kicked, bit, or punched you?"), threat or use of a weapon ("has anyone threatened you with, or actually used, a knife, gun, or other weapon to scare or hurt you?"), sexual abuse ("has anyone forced you to have sex when you did not want to?"), and witnessing violence ("have you witnessed a physical or sexual assault against a family member, friend, or other significant person?") over their lifetime and in the past 12 months.
Perceived coercion was assessed with the MacArthur Perceived Coercion Scale (PCS). The PCS includes five true-false items from the MacArthur Admission Experience Survey and was originally developed to assess perceived coercion associated with the process of hospital admission ( 14 ). The wording was modified for the baseline administration to reflect perceived coercion to enter the jail diversion program. Items included, "I felt free to do what I wanted about going to the diversion program," "I chose to go to the diversion program," "It was my idea to go to the diversion program," I had a lot of control over whether I went to the diversion program," and "I had more influence than anyone else on whether I went to the diversion program." At the 12-month interview, participants who received any mental health or substance abuse services responded to PCS items in regard to perceived coercion to receive outpatient services. Cronbach's alpha was .69.
Mental health symptoms were assessed with the Colorado Symptom Index (CSI) ( 15 ), which consists of 14 self-reported mental health symptom items rated on a 5-point frequency scale. Higher scores are associated with greater symptom severity. Cronbach's alpha was .90.
Arrest data 12 months before the target arrest or incident date and 12 months after the release date associated with the target arrest were collected by each of the 13 jail diversion programs and submitted to the coordinating center. Data on mental health and substance abuse service use were available for six of the 13 jail diversion sites. These data were collected by the diversion program for six months postbaseline for outpatient services and 12 months postbaseline for hospitalizations and emergency department use.
Statistical analyses
Simple two-way associations between each predictor variable and the dependent variables were conducted. The five items regarding perceived coercion to enter the jail diversion program were summed, with a mean score of 1.4±1.4 and a possible range of 0 to 5 points. Higher scores indicate greater perceived coercion. Because the scores on the PCS were not normally distributed, an ordinal variable was created with three levels: highly coerced, moderately coerced, and not coerced. Participants were categorized as highly coerced if they answered "false" to four or five of the five items, moderately coerced if they answered "false" to two or three of the items, and not coerced if they indicated that four or five of the items were true.
Potential predictors of coercion to enter the jail diversion program (baseline) or to receive behavioral health services (12-month) included characteristics of the violation, such as charge type (drug offense, minor offense, or an offense involving another person, violence, or sex), and charge level of the index violation (misdemeanor, felony, or violation), point of diversion (at booking or on parole or probation violation), days from arrest to diversion (quartiles), and number of previous arrests; demographic variables, including age (dichotomized at age 35), gender, black race, Hispanic ethnicity, income (dichotomized at the median of $596 per month), employment status, education (dichotomized at 12 years), and housing status (has housing or lives in a shelter or on the street); clinical variables, such as diagnosis (schizophrenia, bipolar disorder, depression or anxiety disorder, or other) and severity of symptoms on the CSI (in quartiles); substance abuse status (nonuser of drugs or alcohol, moderate user or abuser, or heavy abuser); and exposure to violence (indicator of witnessed violence in past 12 months and indicator of lifetime witnessed violence, indicator of physical violence victimization in past 12 months and indicator of lifetime physical violence victimization, indicator of sexual abuse in past 12 months and indicator of lifetime sexual abuse, and sum of traumatic life events in past 12 months and sum of lifetime traumatic events).
Interactions chosen a priori for investigation were the interactions between race and gender, sexual abuse and gender, physical abuse and gender, sexual abuse and drug use, and physical abuse and drug use. The race-by-gender interaction term was chosen because past research has indicated Caucasian women are most likely to be diverted ( 3 ). Interaction terms of gender with physical or sexual abuse were chosen because of the potential for the abuse variables to measure vastly different experiences for women and men. We chose to examine the possible interaction of physical and sexual abuse with substance abuse because a history of sexual abuse or posttraumatic stress disorder is associated with reporting more coercive experiences in the psychiatric setting ( 16 ) and because the greater mental illness severity found among individuals with a history of interpersonal abuse and also substance abuse problems was assumed to amplify the effects of the interpersonal abuse on coercion. No other interactions were considered.
A random-effects model was used to account for the potential correlation between participants at each site. The SAS GLIMMIX procedure was used with a multinomial response distribution, cumulative logit link function, and maximum likelihood estimation in order to model the dependent variables—coercion to enter the diversion program and coercion to receive behavioral health services. The proportional odds model was selected for the ordinal coercion outcomes after testing in a saturated model whether the fit of the generalized logistic model was superior. Starting with a model containing all main effects and the a priori selected interactions, a stepwise model selection procedure was implemented. To model outpatient service counts, we used a random-effects model with a negative binomial distribution and log link. Backward selection was used to select a final model.
Results
Participants
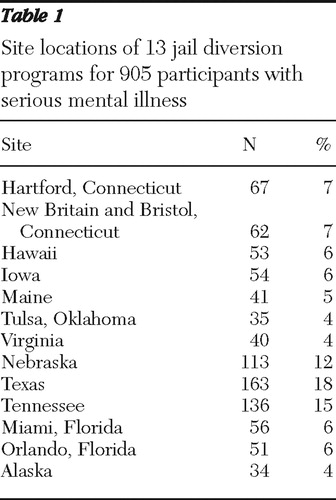
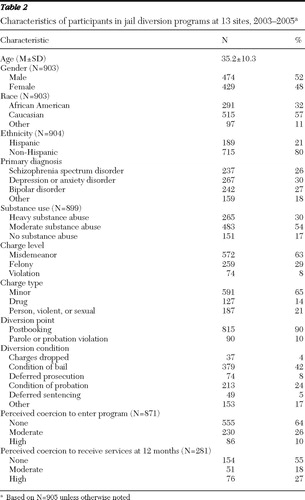
The distribution of participants at the 13 sites is shown in Table 1 . Just over half of the participants were male (52%), 32% were African American, and 21% were Hispanic ( Table 2 ). The most common diagnoses were depression and anxiety disorders (30%), followed by bipolar disorder (27%), schizophrenia spectrum disorders (26%), and other disorders (18%). Eighty-four percent of the sample reported moderate to heavy substance use, and 55% (N=500) had been sexually abused in their lifetime. Most of the participants were arrested on a misdemeanor charge (63%) and diverted as a condition of bail (42%) or probation (24%).
 |
 |
Perceived coercion to enter the jail diversion program
A total of 905 participants completed the baseline interview. Thirty-four of these individuals had at least one item missing from the PCS, resulting in 871 participants with complete responses. Ten percent reported a high level of perceived coercion, 26% reported moderate coercion, and 64% reported no coercion. Significant unadjusted relationships were found for coercion and race-ethnicity ( χ2 =14.52, df=4, p=.01) and coercion and substance abuse ( χ2 =12.5, df=4, p=.001). Specifically, higher levels of coercion were more likely to be reported by African Americans and those reporting high levels of substance abuse.
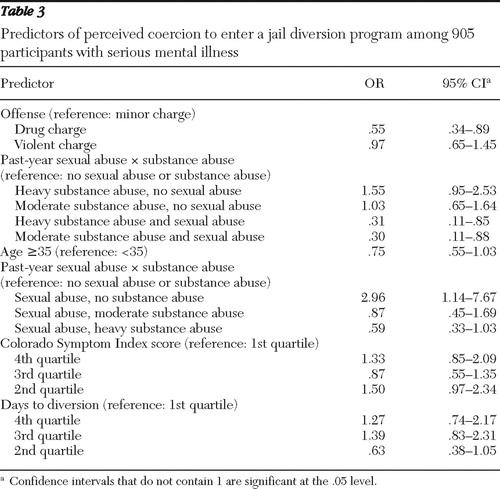
Results of the best-fitting proportional odds model are summarized in Table 3 . Individuals with a drug charge were significantly less likely to report higher levels of coercion than individuals with a minor charge, although risk of reporting coercion did not differ between individuals with a minor charge and those with a violent charge. Specifically, individuals with a drug charge were about half as likely as individuals with a minor charge to report moderate coercion versus no coercion (or to report high coercion versus moderate coercion). The association between past-year sexual abuse and perceived coercion depended on the level of substance abuse; that is, sexual abuse was associated with an increased likelihood of reporting higher levels of coercion but only among those with no current substance abuse. Among participants with no current substance abuse, those reporting sexual abuse in the past year had 2.96 times greater odds of reporting moderate coercion versus no coercion (or of reporting high coercion versus moderate coercion) than individuals who reported no sexual abuse in the past year. Although CSI symptoms and time spent in jail before entering the diversion program were both associated with coercion ( Table 3 ), there was no monotonic relationship between these variables and reported level of coercion.
 |
Perceived coercion to receive behavioral health services
Forty-four percent (N=398) of the baseline sample participated in the 12-month interviews. This substantially reduced 12-month sample differed from the baseline sample on several variables. They were more likely to be female and 35 years of age or older. They were less likely to be Hispanic, employed, or to have a drug charge or a diagnosis of a bipolar disorder. The 12-month sample did not differ from the baseline sample on baseline coercion score. Therefore, despite the possibility of selection bias, we chose to report these results. Only participants who reported receiving any outpatient services were asked the PCS items with regard to receipt of behavioral health services, resulting in a sample of 281 participants. The PCS rating for the 281 participants was 1.03±1.4. A total of 27% of responses were categorized as high coercion, another 18% moderate coercion, and 55% no coercion ( Table 2 ). Unadjusted models for coercion to receive behavioral health services found associations with charge level ( χ2 =11.33, df=4, p=.02), homelessness ( χ2 =6.04, df=2, p=.05), days to diversion ( χ2 =12.52, df=6, p=.05), and baseline level of reported coercion to enter the program ( χ2 =19.94, df=4, p=.001). Individuals charged with a misdemeanor were less likely than those with a felony or violation to report feeling coerced into using behavioral services. Homeless individuals were less likely to report high coercion but were more likely to report moderate coercion than their nonhomeless counterparts. Finally, individuals who reported moderate coercion at baseline were more likely to report higher coercion to receive services at the 12-month interview.
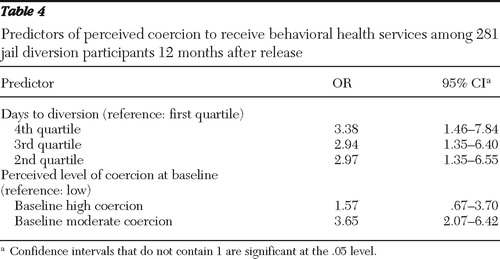
Results of the best-fitting multivariate proportional odds model are summarized in Table 4 . Individuals with longer delays to diversion had increased odds of reporting a higher level of coercion to receive behavioral health services, with individuals in the second quartile having 2.97 times the odds of reporting a higher level of coercion (moderate versus none or high versus moderate) compared with individuals in the first quartile. Individuals in the third quartile had 2.94 times the odds of reporting a higher level of coercion than individuals in the first quartile, and individuals in the fourth quartile had 3.38 times the odds of reporting a higher level of coercion than individuals in the first quartile. Finally, participants who reported moderate levels of coercion at baseline had 3.65 times the odds of reporting higher levels of coercion to receive services at 12 months, although individuals reporting high levels of coercion at baseline were not significantly more likely to report higher levels of coercion to receive services at 12 months.
 |
Effect of coercion on behavioral health service use
Service use data were obtained for six of the 13 sites (N=348). The most common services included case management (92%, N=320), outpatient services other than case management (89%, N=309), and medication management (61%, N=213). A random-effects model of outpatient service use that controlled for demographic, clinical, and criminal justice factors indicated no significant relationship between coercion to enter the jail diversion program and the number of behavioral health service visits. However, older participants had 1.26 (95% confidence interval [CI]=1.05–1.51) times the outpatient service counts as younger participants. Hispanic males had .50 (CI=.27–.93) times the service counts as Hispanic females. Participants with the highest symptom severity had 1.35 (CI=1.04–1.75) times greater service counts than those with the lowest symptom severity. Those reporting lifetime sexual abuse but no substance abuse and no history of physical abuse had 1.84 (CI=1.21–2.78) times the outpatient service counts compared with those not reporting sexual abuse. Those with physical abuse but no sexual abuse or substance abuse had .54 (CI=.32–.88) times the service counts as those with no interpersonal abuse and no substance abuse.
Discussion
We found that most participants in this study did not feel coerced to enter the jail diversion program or to receive behavioral health services during the year after diversion. Ten percent of the sample reported high coercion and 26% reported moderate coercion into entering the jail diversion program. Responses regarding the receipt of services at the 12-month interview indicated that 27% perceived a high level of coercion and 18% perceived a moderate level. These levels of perceived coercion reported among jail diversion participants are actually no greater than those reported by voluntary psychiatric outpatients ( 10 ) or participants in a mental health court ( 17 ) and are considerably lower than the levels of coercion reported among some samples of involuntary psychiatric inpatients ( 8 , 18 ) or psychiatric outpatients ( 10 ).
Participants with a drug charge were less likely to report higher levels of perceived coercion. Presumably, people facing drug charges (compared with minor charges) may have greater incentive to consider alternatives to incarceration and therefore view the diversion program as a positive choice. Experiencing sexual abuse in the past 12 months was associated with higher levels of perceived coercion but only among non-substance abusers. In other words, sexual abuse may lead an individual to feel a lack of control and possibly greater sensitivity to coercion, but this is no longer true when the person engages in substance abuse (and possibly faces drug-related charges).
One year after a person's enrollment in the jail diversion program, the only variables that explained level of perceived coercion to receive behavioral health services were higher level of baseline coercion and longer wait from arrest to diversion. These findings must be interpreted cautiously in view of the substantial attrition rate (56%) from baseline to the 12-month interview.
An important question this study sought to address is whether feeling coerced would lead to poorer engagement in services and lower overall levels of service contact. We found no evidence to support this hypothesis. Factors that predicted service use included older age, higher symptom severity, and lifetime history of sexual abuse among those without a history of physical abuse or current substance abuse. On the other hand, male gender among Hispanics and experiencing physical abuse without a history of sexual abuse or substance abuse were associated with fewer outpatient visits.
A significant strength of the study is that the findings are based on data from a large, multisite jail diversion initiative. A number of important limitations also exist. Although the study identified characteristics that were associated with perceived coercion, its design did not permit a full explanation of why participants might have felt coerced. Questions regarding the process of diversion, including the role of participants' views of procedural justice, negative pressures, comprehension of the voluntary nature of their participation, and the perceived need for treatment, would provide a more thorough understanding of coercion in jail diversion. Each of these variables has been found to be associated with level of perceived coercion in previous research involving persons with mental illness in other settings ( 19 , 20 , 21 ) and should be further explored in future studies of jail diversion.
Conclusions
Most participants in this multisite study did not perceive coercion in the jail diversion process. Further, perceived coercion was unrelated to the overall level of service use. Additional research is needed to further understand coercion in jail diversion programs by examining the perceived need for treatment among participants, negative pressures placed on participants, and their views of procedural justice.
Acknowledgments and disclosures
This research was supported in part by grant K01MH079343 from the National Institute of Mental Health, and by the Center for Mental Health Services, Substance Abuse and Mental Health Services Administration (1-H79-SM-54722-01).
The authors report no competing interests.
1. Steadman HJ, Osher FC, Robbins PC, et al: Prevalence of serious mental illness among jail inmates. Psychiatric Services 60:761–765, 2009Google Scholar
2. Criminal Justice and Mental Health Consensus Project. New York, Council of State Governments Eastern Regional Conference, 2002Google Scholar
3. Steadman HJ, Naples M: Assessing the effectiveness of jail diversion programs for persons with serious mental illness and co-occurring substance use disorders. Behavioral Sciences and the Law 23:163–170, 2005Google Scholar
4. Lamberti JS, Weisman RL, Schwarzkopf SB, et al: The mentally ill in jails and prisons: towards an integrated model of prevention. Psychiatric Quarterly 72:63–77, 2001Google Scholar
5. Lamb RL, Weinberger LE, Reston-Parham C: Court intervention to address the mental health needs of mentally ill offenders. Psychiatric Services 47:275–281, 1996Google Scholar
6. Steadman HJ, Cocozza JJ, Veysey BM: Comparing outcomes for diverted and nondiverted jail detainees with mental illnesses. Law and Human Behavior 23:615–627, 1999Google Scholar
7. Watson AC, Angell B: Applying procedural justice theory to law enforcement's response to persons with mental illness. Psychiatric Services 58:787–793, 2007Google Scholar
8. Hiday V, Swartz M, Swanson J, et al: Patient perceptions of coercion in mental hospital admission. International Journal of Law and Psychiatry 20:227–241, 1997Google Scholar
9. Nicholson RA, Ekenstam C, Norwood S: Coercion and the outcome of psychiatric hospitalization. International Journal of Law and Psychiatry 19:201–217, 1996Google Scholar
10. Swartz MS, Hiday VA, Swanson JW, et al: Measuring coercion under involuntary outpatient commitment: initial findings from a randomized controlled trial. Research in Community Mental Health 10:57–77, 1999Google Scholar
11. Kaltiala-Heino R, Välimäki M: Involuntary psychiatric treatment in the threshold of the 21st century. Psychiatria Fennica 30:185–204, 1999Google Scholar
12. Rain S, Steadman H, Robbins P: Perceived coercion and treatment adherence in an outpatient commitment program. Psychiatric Services 54:399–401, 2003Google Scholar
13. Rain S, Williams V, Robbins P, et al: Perceived coercion at hospital admission and adherence to mental health treatment after discharge. Psychiatric Services 54:103–105, 2003Google Scholar
14. Gardner W, Hoge SK, Bennett N, et al: Two scales for measuring patients' perceptions for coercion during mental hospital admission. Behavioral Sciences and the Law 11:307–321, 1993Google Scholar
15. Shern DL, Wilson NZ, Cohen AS, et al: Client outcomes: II. longitudinal client data from the Colorado Treatment Outcome Study. Milbank Quarterly 72:123–143, 1994Google Scholar
16. Frueh BC, Knapp RG, Cusack KJ, et al: Patient safety within the psychiatric setting. Psychiatric Services 56:1123–1133, 2005Google Scholar
17. Poythress N, Petrila J, McGaha A, et al: Perceived coercion and procedural justice in the Broward mental health court. International Journal of Law and Psychiatry 25:517–533, 2002Google Scholar
18. Hogue SK, Lidz CW, Eisenberg M, et al: Perceptions of coercion in the admission of voluntary and involuntary psychiatric patients. International Journal of Law and Psychiatry 20:167–181, 1997Google Scholar
19. Elbogen E, Swanson J, Swartz M: Effects of legal mechanisms on perceived coercion and treatment adherence among persons with severe mental illness. Journal of Nervous and Mental Disease 191:629–637, 2003Google Scholar
20. Farabee D, Shen H, Sanchez S: Perceived coercion and treatment need among mentally ill parolees. Criminal Justice and Behavior 29:76–86, 2002Google Scholar
21. McKenna B, Simpson A, Coverdale J: Outpatient commitment and coercion in New Zealand: a matched comparison study. International Journal of Law and Psychiatry 29:145–158, 2006Google Scholar

