
Treatment Receipt by Veterans After a PTSD Diagnosis in PTSD, Mental Health, or General Medical Clinics
To address the complex mental health needs of veterans with posttraumatic stress disorder (PTSD), the Department of Veterans Affairs (VA) has established over 300 inpatient and outpatient specialty treatment programs ( 1 , 2 ). Despite the availability of these specialty services, a recent evaluation of VA mental health services concluded that service provision in the VA has not kept pace with demand for PTSD services ( 1 ). Furthermore, the authors of the evaluation report speculated that among those who obtained treatment, inadequate appointment frequency might contribute to premature termination ( 1 ). However, to determine how warranted this concern might be, rates of treatment initiation and persistence in treatment would need to be established.
Of the 305,142 veterans who were seen for PTSD in VA facilities in fiscal year (FY) 2006, less than one-third received their treatment in a specialized PTSD program. More than half were seen in general mental health clinics, and another 10% in general medical clinics ( 2 ). In non-VA settings, rates of mental health treatment initiation and persistence in treatment have been shown to vary across treatment sectors. For example, among participants in the National Comorbidity Survey Replication who were treated for PTSD, treatment delivered by mental health specialists (for example, psychiatrists) was associated with fourfold higher odds of receiving a minimally adequate trial of treatment compared with those who were treated by general medical providers ( 3 ). Other studies have reported similar findings ( 4 , 5 ).
The first goal of this study was to establish rates of treatment initiation and minimally adequate treatment trials among veterans with PTSD. Because the odds of receiving a minimally adequate trial vary across treatment sectors in non-VA populations ( 3 ), our second goal was to determine whether comparable variation exists within the VA. We were particularly interested in whether receipt of a PTSD diagnosis in specialized PTSD programs increased veterans' odds of treatment initiation and whether treatment in such programs increased their odds of receiving a minimally adequate treatment trial over and above that found in general mental health or general medical clinics. The study examined rates of outpatient treatment initiation and receipt of minimally adequate treatment trials among veterans given a new diagnosis of PTSD in VA facilities in 2004–2005.
Methods
We used a retrospective cohort to examine VA treatment initiation and participation in the six months after a new PTSD diagnosis. The study was approved by the institutional review board of the Minneapolis VA Medical Center. Participants were veterans who received a DSM-IV diagnosis of PTSD (309.81) at any VA facility between April 1, 2004, and March 31, 2005. Excluded were veterans with cognitive impairment or psychosis and veterans who had any visits to a VA mental health facility, a prescription for an antidepressant, or a diagnosis of a mental disorder except for substance abuse in the previous year. Pharmacy and appointment data from FY 2003 through FY 2005 were used to identify new episodes of PTSD treatment between April 1, 2004, and March 31, 2005. We chose to include veterans who had substance abuse treatment because the diagnosis of PTSD may not be evident until the primary substance abuse problem is sufficiently addressed ( 6 ).
Measures
There were eight outcome measures. The total number of veterans with a new PTSD diagnosis was used as the denominator, and the four treatment initiation outcomes were the proportion of veterans who received a prescription for a psychiatric medication, the proportion who received a prescription for an antidepressant, the proportion who received any behavioral counseling, and the proportion who received either psychiatric medication or behavioral counseling. To ascertain whether a veteran received a minimally adequate treatment trial, we examined the following three outcomes: among veterans who received any psychiatric medications, the proportion receiving at least four 30-day supplies; among veterans who received any antidepressant prescription, the proportion receiving at least four 30-day supplies; and among veterans who received any counseling, the proportion receiving at least eight counseling visits. Outcomes were coded as present or absent for each participant. These criteria for a minimally adequate treatment trial have been used by others ( 7 ) and are consistent with treatment guidelines ( 8 ). At the time these data were collected, the VA had not yet begun its rollout of evidence-based psychotherapy interventions, which require ten or 12 visits ( 11 ). The eighth outcome was the number of PTSD-related appointments in any treatment sector within the six-month period after the index appointment.
We used a VA administrative database, the National Patient Center Database (NPCD), to obtain demographic, diagnostic, and visit information for the six months after an index PTSD visit. Visit information included number and CPT codes of visits with a diagnosis of PTSD. CPT codes 90804–90809, 90846, 90847, 90853, 90862, 90880, 90901, 96152–96154, 99214, 99215, S9445, and S9446 identified counseling appointments. Visits associated with disability examinations were omitted from the analyses. Visits in which the CPT code reflected psychological assessment were used only as index visits and were not counted as treatment visits in the follow-up period.
Information about medication type and amount and number of refills was extracted from the VA's Decision Support Systems (DSS) database. Included were all psychotropic medications of the following classes: antidepressants, antipsychotics, hypnotics or benzodiazepines, mood stabilizers, and stimulants. The DSS pharmacy data set includes prescription details, such as unit dose, number of tablets, and prescription duration. All prescriptions were transformed into 30-day equivalents, such that a 90-day prescription was changed to three one-month supplies and a two-week prescription became .5 of a one-month supply.
Independent variables extracted from the NPCD included demographic information, military variables (prisoner of war [POW] status and service era), disability levels (VA disability status and score on the Charlson Comorbidity Index [CCI] [9]), and factors affecting treatment access (treatment sector, copayment status, category of the veteran's primary residence according to population density, census division, and distance from the nearest VA facility). The CCI is a measure of mortality risk determined from the presence or absence of specific medical comorbidities ( 9 ) and thus reflects the relative burden of severe medical problems. The CCI was constructed from diagnostic information from FY 2003 through 2005. Treatment sector—the VA sector in which the veteran received the PTSD diagnosis (index clinic type: general medical clinic, mental health clinic, or PTSD specialized program) was the primary variable of interest. Index clinic type was determined by the stop code (an administrative indicator) of the visit in which a PTSD diagnosis first occurred. Stop code assignment to the three treatment sectors was similar to that used by the Northeast Program Evaluation Center ( 2 ).
Analyses
We used logistic regression for all dichotomous outcomes and negative binomial regression for number of PTSD-related visits to examine the independent effect of treatment sector on study outcomes after controlling for other covariates and potential confounders. Generalized estimating equations accounted for clustering by facility. Analyses were conducted in the GENMOD procedure of SAS, version 9.1 ( 12 ), with working correlation compound symmetry, type 3 score tests for effects, and confidence intervals computed on the logit or log rate scales by the Wald method with empirical standard errors. Estimates are least-squares means computed on the logit or log rate scale; they and confidence intervals were back-transformed to the original scale.
The following predictors were entered into the regression models: race (Asian American, Native American, black, Hawaiian or Pacific Islander, white, multiracial, and unknown race), ethnicity (Hispanic, non-Hispanic, and unknown ethnicity), gender, age, marital status, period of service (pre-Vietnam, Vietnam, post-Vietnam), POW status (former POW, non-POW, and unknown POW status), degree of service-connected disability (not service connected, 20% service connected or less, 30%–40%, 50%–60%, and 70% or more), CCI score, distance from a VA facility in quartiles (≤9.34 miles, >9.34 and ≤24.92 miles, >24.92, ≤55.96 miles, and >55.96 miles), U.S. census-defined population density of primary residence (urban, urban fringe, and rural), census division, VA copayment status (copayment, no copayment, and no copayment or cost-sharing agreement), and treatment sector (general medical clinic, mental health clinic, and PTSD specialized program).
Index clinic type was considered to be a significant predictor only if it remained significant after entry of all other variables. When index clinic type was significant, Wald statistics and odds ratios were used to make comparisons between groups. Simple chi square tests were used to test the association between index clinic type and treatment sectors of visits during the follow-up period and between number of follow-up visits and number of 30-day prescriptions of psychotropic medications received.
Results
Table 1 presents data on demographic and other characteristics of the sample. Most of the veterans in the sample were male (96%), and whites accounted for 44% of the sample. The mean age was 55.2 years.
 |
Of the 215,442 veterans who received a PTSD diagnosis in a VA facility during the study period, 21% (N=46,053) had no mental health visits during the previous year (other than for substance abuse treatment). After exclusion of veterans who had cognitive impairments, who had received any mental health diagnosis not related to substance abuse, or who had any antidepressants in the prior year, 9% (N=20,284) met inclusion criteria. Of these 20,284 veterans, 4,336 received a PTSD diagnosis in a PTSD specialty clinic, 11,169 in a mental health clinic, and 4,779 in a general medical clinic.
Of these 20,284 veterans, 50% (N=10,127) were prescribed a psychotropic medication, and 39% (N=7,980) received some counseling. Sixty-four percent (N=13,028) received some treatment—either medication or counseling. About half of the veterans prescribed medication (54%, N=5,487) received at least four one-month supplies. Only 24% (N=1,909) of those who received any counseling had at least eight counseling sessions. In all, 33% (N=6,616) of those who received a diagnosis of PTSD received a minimally adequate treatment trial in the subsequent six months. The low rates were not related to large numbers of new users entering the VA system, because differences in outcome measures between new and established VA users were not significant.
Of veterans who received any medication, 80% (N=8,093) received antidepressants, 15% (N=1,526) antipsychotics, 19% (N=1,894) mood stabilizers, 23% (N=2,301) hypnotics or benzodiazepines, and <1% (N=31) stimulants. Veterans prescribed antidepressants were most likely to receive medication for at least four months (44%, N=3,571), and those prescribed antipsychotics were least likely to receive a four-month supply (25%, N=387) ( χ2 =185.8, df=1, p<.001). The mean±SD number of counseling appointments among those who received any counseling was 5.7±7.3.
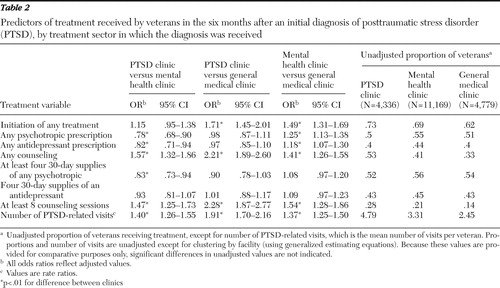
Table 2 shows differences in mental health treatment according to the treatment sector in which veterans received a PTSD diagnosis, after adjustment for all other predictors of mental health service use. Differences across sectors were most evident for initiation of specific types of treatment. For example, the odds of receiving counseling services were highest for veterans given a diagnosis in a PTSD program, and the odds of receiving pharmacotherapy were highest for those given the diagnosis in a mental health clinic. Similarly, the odds of receiving at least eight counseling sessions were better for those initially seen in a PTSD clinic. In contrast, the odds of receiving at least four 30-day supplies of antidepressants did not differ by type of index clinic. The importance of follow-up visits of any type was demonstrated by the fact that the odds of receiving four or more 30-day supplies of psychotropic medications increased as the number of follow-up visits increased ( χ2 =4,418.9, df=4, p<.001). More specifically, among the 5,487 veterans who received at least four 30-day supplies of psychotropic medications, 42% (N=2,277) had five or more follow-up visits, compared with only 26% (N=1,227) of the 4,640 veterans who received less medication and only 11% (N=1,137) of the 10,157 veterans who received none. [A table presenting odds ratios and rate ratios for the covariates is available as an online supplement to this article at ps.psychiatryonline.org .]
 |
Given the limitations of our administrative data, we could not ascertain from which type of clinic prescriptions were given. We could, however, compare index clinic types according to the distribution of PTSD-related visits after the index visits. Distribution of these visits differed by index clinic type ( χ2 =19,158.9, df=4, p<.001). For veterans who received an initial diagnosis in a PTSD clinic, more of their follow-up visits were to PTSD clinics (N=19,647, 76%) than to mental health clinics (N=4,141, 16%) or primary care clinics (N=1,027, 4%). Follow-up visits for those who received a diagnosis in a mental health clinic were more likely to be to mental health clinics (N=25,200, 58%) than to PTSD clinics (N=13,243, 31%) or primary care clinics (N=3,167, 7%). In contrast, follow-up visits of those who received a diagnosis in a primary care clinic were more likely to be to other sectors—most often to mental health clinics (N=5,407, 40%), followed by PTSD clinics (N=4,315, 32%) and primary care clinics (N=3,247, 24%). (Percentages of follow-up visits do not add to 100 because some visits occurred outside of the three treatment sectors.)
We also examined how many of the PTSD-related follow-up visits were for counseling and whether the odds of follow-up visits for counseling were similar for the three treatment sectors. For veterans given a diagnosis in a PTSD clinic, 69% (N=13,626) of all follow-up visits to PTSD clinics were for counseling compared with 38% of follow-up visits to mental health clinics (N=1,580) and 24% of visits to primary care (N=244) ( χ2 =10,700, df=4, p<.001). For those given a diagnosis in a mental health clinic, 45% of all follow-up visits in mental health clinics were for counseling (N=11,267) compared with 69% of their visits to PTSD clinics (N=9,089) and 23% of visits to primary care clinics (N=739). Finally, for those who received a diagnosis in a primary care clinic, 35% of subsequent primary care visits were for counseling (N=1,121) compared with 60% of visits to PTSD clinics (N=2,576) and 35% of visits to mental health clinics (N=1,897).
Discussion
Of veterans who were given a diagnosis of PTSD, only about two-thirds received some VA mental health care in the six months after the diagnosis. Only about half of those who received any mental health care received a minimally adequate treatment trial. These rates are similar to those reported for depression treatment in other populations ( 4 , 5 ).
Consistent with findings in non-VA settings, receipt of a PTSD diagnosis in a mental health clinic conferred some advantage in treatment initiation and receipt of minimally adequate treatment compared with receipt of a PTSD diagnosis in a general medical clinic. Receipt of a diagnosis in a PTSD clinic compared with a general medical clinic conferred even greater advantage in terms of subsequent appointment frequency and provision of counseling. In part, this may be attributable to greater expertise among providers in specialty PTSD programs in engaging patients with PTSD in treatment and providing appropriate counseling services. Alternatively, it may reflect differential odds of being referred to another treatment sector: those who received a diagnosis in a PTSD clinic were less likely than those who received a diagnosis elsewhere to be seen for follow-up in the other two treatment sectors. From this perspective, the lower likelihood of treatment initiation among veterans who received a PTSD diagnosis in primary care may reflect problems in the referral process or a lack of access to specialty PTSD clinics. During the sampling frame of this study, PTSD programs were concentrated in urban areas ( 2 ), whereas primary care clinics had already been established in rural areas as community-based outpatient clinics. Recent efforts to integrate mental health providers into primary care clinics might address this problem. These findings also suggest that recent initiatives to have general medical providers in community-based clinics treat PTSD should be monitored closely to ensure treatment outcomes comparable to those in mental health clinics.
Despite these differences, it should be noted that the observed variation in the odds of treatment receipt across the three treatment sectors, although significant, was not large. For example, only an additional 7% of the veterans who received a diagnosis in a primary care clinic would have initiated some mental health treatment had they received a diagnosis in a mental health clinic during the sampling period. On the other hand, although this difference is fairly small given the size of the overall population, the cumulative effect of small differences over time may contribute to the increasing number of veterans who receive VA disability benefits based on service connection for PTSD.
This study had several limitations. Because we used administrative data, we could not assess whether selection bias across treatment sectors explained our findings. For example, veterans who were willing to be seen by a mental health specialist for an initial diagnostic evaluation may be more accepting of their diagnosis and more willing to accept treatment recommendations. In addition, we do not know whether a veteran who was given a diagnosis in one sector received any or all of his or her medication from that sector because we could not ascertain in which clinic prescriptions were written. More detailed information will be required to determine whether observed differences in treatment reflect differences in treatment quality or problems in the referral process. Use of administrative data also limited our ability to confirm whether veterans with a diagnosis of PTSD actually had PTSD or to determine whether those without a diagnosis of PTSD should have had one. Similarly, we do not know how many received non-VA mental health treatment. Finally, we do not know whether prescribed medications were offered for conditions other than PTSD, such as chronic pain; however, there is no reason to assume that nonpsychiatric use of these drugs would differ across index clinic types.
Conclusions
Approximately one-third of veterans given a diagnosis of PTSD in the VA health system received a minimally adequate treatment trial in the six months after diagnosis. Given the role of treatment nonadherence in the development and maintenance of chronic mental illness ( 10 ), more needs to be done to engage veterans with PTSD to stay in treatment. Treatment by mental health specialists, particularly PTSD specialists, increased the odds of treatment initiation and the frequency of appointments, suggesting that expansion of these specialized services may be required to better address this population's mental health needs. Additional research should examine the relationship between the quality of care and treatment adherence in this population.
Acknowledgments and disclosures
This research was supported by grant IAC 06-266 from VA Health Services Research and Development. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
The authors report no competing interests.
1. Rosenheck RA, Fontana AF: Recent trends in VA treatment of posttraumatic stress disorder and other mental disorders. Health Affairs 26:1720–1727, 2007Google Scholar
2. Fontana A, Rosenheck R, Spencer H, et al: Treatment of Posttraumatic Stress Disorder in the Department of Veterans Affairs: Fiscal Year 2006 Service Delivery and Performance. Long Journey Home series, 15. West Haven, Conn, Department of Veterans Affairs, Northeast Program Evaluation Center, Mar 2007. Available at vaww.nepec.mentalhealth.med.va.gov/PTSD/ptsLJHAF.pdf Google Scholar
3. Wang PS, Lane L, Olfson M, et al: Twelve-month use of mental health services in the United States. Archives of General Psychiatry 62:629–640, 2005Google Scholar
4. Lewis E, Marcus SC, Olfson M, et al: Patients' early discontinuation of antidepressant prescriptions. Psychiatric Services 55:494, 2004Google Scholar
5. Weilburg JB, O'Leary KM, Meigs JB, et al: Evaluation of the adequacy of outpatient antidepressant treatment. Psychiatric Services 54:1233–1239, 2003Google Scholar
6. Kimerling R, Trafton JA, Nguyen: Validation of a brief screen for post-traumatic stress disorder with substance use disorder patients. Addictive Behaviors 31:2074–2079, 2006Google Scholar
7. Harman JS, Edlund MJ, Fortney JC: Disparities in the adequacy of depression treatment in the United States. Psychiatric Services 55:1379–1385, 2004Google Scholar
8. Management of Post-Traumatic Stress. Office of Quality and Performance pub no 10Q-CPG/PTSD-03. Washington, DC, Department of Veterans Affairs, Veterans Health Administration, and Department of Defense, Office of Health Affairs, Dec 2003Google Scholar
9. Deyo R, Cherkin D, Ciol M: Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. Journal of Clinical Epidemiology 45:613–619, 1992Google Scholar
10. Jacobson N, Greenley D: What is recovery? A conceptual model and explication. Psychiatric Services 52:482–485, 2001Google Scholar
11. Monson CM, Schnurr PP, Resick PA: Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. Journal of Consulting and Clinical Psychology 74:898–907, 2006Google Scholar
12. SAS 9.1 Release. Cary, NC, SAS Institute, 2009. Available at support.sas.com/onlinedoc/913/docMainpage.jsp Google Scholar

