
Risk Factors for Homelessness: Evidence From a Population-Based Study
One of the most pressing social issues facing the United States and other Western countries is the high rate of homelessness ( 1 , 2 , 3 ). It is estimated that 3.5 million Americans in any given year experience homelessness ( 1 ). It is important to understand the causes of homelessness because poorly informed service delivery for homeless populations may be ineffective or, worse, counterproductive ( 3 , 4 ).
The physical and mental health of people who are homeless is considerably worse than that of the general population ( 5 , 6 , 7 ). The prevalence of mental disorders is three to four times higher among the homeless population, with rates of affective and anxiety disorders and drug and alcohol abuse particularly elevated ( 8 , 9 , 10 , 11 , 12 ). Rates of DSM diagnoses among the homeless are almost double those among persons who have never been homeless, whereas the rate of alcohol use disorder co-occurring with one or more psychiatric disorders has been identified as five times greater ( 13 ). Homelessness is also associated with a high risk of suicide attempts ( 14 ).
Previous research has shown that so-called biographical risk factors are important to understanding the pathways into homelessness ( 8 , 15 ). Specifically, a disproportionate number of homeless people report experiences of childhood adversity, including poor relationships with parents, neglect, physical and sexual abuse, and being forced or placed out of the home ( 15 , 16 , 17 ). One study indicated that up to 50% of homeless and runaway adolescents may have experienced physical abuse; almost one-third reported sexual abuse ( 18 ). These experiences may contribute to the risk of mental health problems both concurrently and later in life ( 19 , 20 , 21 ).
Other factors that have been reported to contribute to risk of homelessness are school expulsion and lack of academic qualifications, poor social networks, and antisocial and offending behavior (including experiences in prison) ( 5 , 22 , 23 ). With important exceptions ( 13 , 24 ), however, most of the research on the etiology of homelessness has been conducted in service settings, including shelters and rehabilitation centers, or with psychiatric patients (current or with a history of admission to a psychiatric hospital) ( 25 , 26 , 27 ). These samples are likely to underrepresent those who are homeless for short periods or do not belong to a specific subgroup of homeless individuals ( 28 ). Choice of sampling site will also influence prevalence rates (such as regional socioeconomic and political differences and exclusion criteria used by service providers) ( 29 ). Finally, homelessness has complex and multifactorial origins. With exceptions ( 13 , 24 ), many studies of homelessness have focused on a limited selection of risk factors and have not also considered the relative role of a wide range of possible risk factors.
Our study used a large, representative, population-based sample to evaluate relationships between well-established factors (previously identified in smaller and non-population-based samples as potentially important to understanding the etiology of homelessness) and lifetime homelessness status and the relative importance of these factors in the prediction of homelessness.
Methods
Sample
The sample used in this study was derived from the National Longitudinal Study of Adolescent Health (Add Health) a project designed by Udry, Bearman, and Harris ( 30 , 31 ). The primary sampling frame included all high schools in the United States with an 11th grade and at least 30 enrolled students. From this pool, a systematic random sample of high schools was selected. A clustered sampling design was used to ensure that the sample (134 high schools) was representative of high schools in the United States with regard to region, urbanicity, school type, size, and racial and ethnic composition of the student body. A random sample of students was selected to take part in computer-assisted interviews at home.
Respondents were recruited in 1994–1995, when they were 11–18 years old. Eligibility at this stage was based on whether respondents were listed on grade enrollment rosters. Respondents were recontacted one year later (1996) and six years later (2001), when they were young adults (age range 18–28 years; mean±SD=21.97±1.77). Our study used data collected in 2001 (wave 3), during which information was obtained on homelessness as well as experiences of severe childhood adversity. Of persons who were recontacted for the third wave of data collection, 15,170 completed an interview (response rate 76%). After a complete description of the study was presented to respondents, their written informed consent was obtained. Most interviews (80%) were conducted at or just outside the respondent's residence or at the respondent's parents' residence (when the respondent had a separate residence; 8%). The remaining interviews took place in the interviewer's car or at another location. All phases of the Add Health study have been approved by the Public Health Institutional Review Board of the Office of Human Research Ethics. We used data from respondents who provided information about their homelessness status at wave 3 (N=14,888).
Measures
Measures were developed for the Add Health In-Home Adolescent Interview and were piloted extensively before being used as part of the survey ( 30 , 31 , 32 ). For our study, inclusion as homeless was based on responses to three questions: "Have you ever been homeless for a week or longer—that is, you slept in a place where people weren't meant to sleep, or slept in a homeless shelter, or didn't have a regular residence in which to sleep?" "Have you ever stayed in a homeless shelter?" and "Where do you live now? That is, where do you stay most often? Response options include 'Homeless'—that is, you have no regular place to stay."
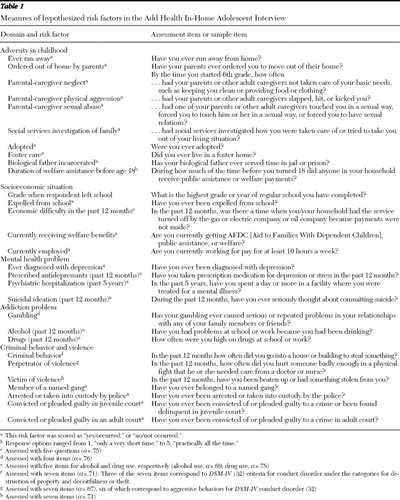
Sample items regarding the assessment of each hypothesized risk factor are presented in Table 1 , and additional information can be found elsewhere ( 32 ). For ease of interpretation, items are grouped into five domains: childhood adversity, socioeconomic situation, mental health problems, addiction problems, and criminal behavior and violence. Seven of these factors comprised multiple items, each of which demonstrated acceptable internal consistency (Cronbach's α >.69).
 |
Statistical analysis
Analyses proceeded in three stages. First, the group with a history of homelessness was compared on each individual hypothesized risk factor with the group of respondents who had never been homeless. Second, the pattern of associations among hypothesized risk variables was examined. Third, the risk factors were assessed simultaneously with logistic regression to evaluate the subset of factors that best predicted homelessness. The regression analyses also accounted for the effects of age ( 33 ), gender ( 34 ), and race and ethnicity ( 35 , 36 , 37 ), partly in light of previous research showing links between these factors and homelessness. The univariate analysis and logistic regression were repeated with a sample-weights statement (in the Stata software) ( 38 ). This procedure corrects for design effects and unequal probability of selection to ensure that the results are nationally representative, with unbiased estimates. The construction of the sample weights includes an adjustment for nonresponse ( 31 ).
Results
We used data from 14,888 respondents (men, 7,037; women, 7,851) who provided information about their homelessness status at wave 3. The racial and ethnic distribution of the sample was approximately 67% Caucasian (N=9,899), 23% black or African American (N=3,376), 16% Hispanic (N=2,416), 8% Asian or Pacific Islander (N=1,253), and 6% Native American (N=815). Respondents were able to endorse more than one racial-ethnic group
A total of 682 respondents (4.6% of the sample; 354 men and 328 women) were classified as ever being homeless (610 respondents had been homeless for a week or longer, 199 had stayed in a homeless shelter, and six respondents were homeless during the wave 3 interview). Preliminary analyses of demographic factors indicated that older age (odds ratio [OR]=1.08, 95% confidence interval [CI]=1.02–1.14) and Native American ethnicity (OR=2.80, CI=1.94–2.41) were significantly associated with homelessness (p<.01).
Univariate analyses
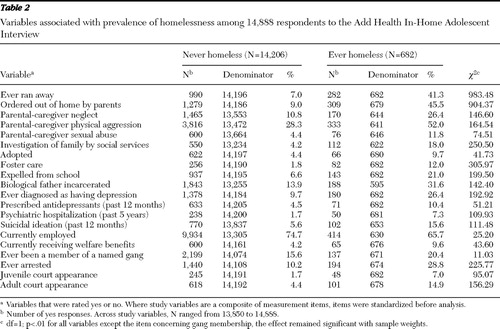
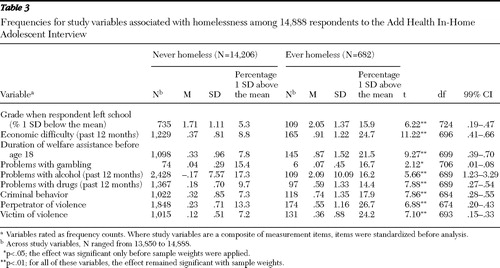
Prevalence rates for each risk factor hypothesized to be associated with homelessness were generally greater in the ever-homeless group compared with the never-homeless group ( Tables 2 and 3 ). The ever-homeless group had elevated levels of parental-caregiver abuse or neglect, and the proportion of ever-homeless respondents who reported that their family had been investigated by social services by the time the respondent reached sixth grade was four times greater ( Table 2 ). Almost half of the ever homeless reported having run away or being ordered out of their homes by their parents, and rates of adoption and fostering placements were also higher than in the never-homeless group. A large proportion of respondents in both samples were currently employed, although the rate was higher in the group who had never been homeless. There were higher levels of involvement in crime (as victim or perpetrator) and in the criminal justice system in the group who had experienced homelessness ( Table 3 ). When sample weights were applied, all of the study variables, with the exception of gambling behavior and membership in a gang, were associated with homelessness.
 |
 |
Intercorrelations among study variables
Examination of the pattern of correlations among the hypothesized risk factors indicated some interesting associations between domains of functioning and life experiences. [A table showing the intercorrelations is available as an online supplement to this article at ps.psychiatryonline.org .] Associations were found among the indicators of abuse (both sexual and physical), neglect, and investigation of the family by social services (r=.18–.29, p<.01). Positive associations were found among the four indicators of mental illness (r=.14–.56, p<.01) and between addiction problems (drugs, alcohol, or both) and criminal behavior (r=.29–.39, p<.01). Weak positive associations were found between the physical and sexual abuse variables and mental health problems (r=.05–.12, p<.01) and drug problems (r=.08–.12, p<.01). The variable assessing whether a parent-caregiver had ever ordered the respondent out of his or her home was associated with drug and alcohol problems and the indicators of criminal behavior (r=.10–.14, p<.01). The other indicators of childhood adversity (abuse, neglect, and investigation by social services) were associated with criminal behavior, perpetration of violence, and being a victim of violence (r=.06–.15, p<.01).
Multivariate logistic regression
The multivariate logistic regression revealed several factors that were uniquely associated with homelessness ( Table 4 ). The first set of variables could be broadly classified as childhood adversity: ever having run away from home (OR=4.03), ever having been ordered out of the home by parents (OR=3.16), placement in foster care (OR=2.15), incarceration of the biological father (OR=1.45), parental-caregiver neglect (OR=1.47), and duration of welfare assistance to the family before age 18 (OR=1.14). A second domain reflected socioeconomic situation: grade when the respondent left school (OR=.88), recent economic difficulty (OR=1.23), and current employment (OR=.76). A third domain of problems reflected aspects of mental illness and addiction, including a diagnosis of depression (OR=1.61), having had a psychiatric hospitalization in the past five years (OR=1.82), and problems with drugs in the past 12 months (OR=1.16). Factors not associated with homelessness included parent physical aggression and sexual abuse, investigation of the family by social services, expulsion from school, current recipient of welfare benefits, prescription medication for antidepressants, suicidal ideation, and problems with gambling and alcohol. None of the indicators of criminal behavior or violence were independently associated with homelessness.
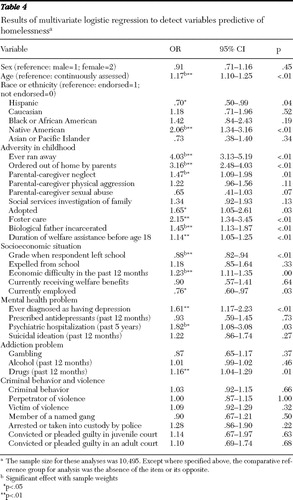 |
Analyses were repeated with sample weights to correct for design effects and unequal probability of selection. Associations with homelessness were retained for the following variables: ever having run away, ordered out of the family home, parental-caregiver neglect, incarceration of the biological father, grade when respondent left school, recent socioeconomic difficulty, and psychiatric hospitalization in the past five years.
Discussion
The findings show that childhood adversity in its various guises is significantly associated with homelessness among young adults. Other factors significantly and independently related to homelessness included economic disadvantage, mental illness (depression and psychiatric hospitalization), and recent drug use. In highlighting the association between childhood experiences and homelessness when assessed in the context of an array of other possible risk factors, the findings have important implications for the prevention of homelessness as well as intervention and service provision.
In assessing the role of a range of factors related to childhood adversity, our findings indicated that events that capture the separation or exit of a child from his or her family or from a parent (being ordered to leave home, running away, being placed in foster care, and having a biological father who was incarcerated) were most strongly associated with homelessness. These results, obtained in a population-based data set, are in agreement with findings from earlier studies based on more highly selected samples ( 5 , 8 , 16 , 39 ). It is noteworthy that indicators of separation from parents or caregivers subsumed other adverse events that were included as risk factors in this study (physical and sexual abuse). This does not necessarily mean that the separation experiences were causal. Rather, they may be regarded as proxy indicators of dysfunctional family processes (including abuse) and individual problems that increased the likelihood of homelessness ( 8 , 25 , 39 ).
Neglect and adoption were also linked to homelessness, but less strongly than other factors (p<.05). It might seem paradoxical that our findings indicate that risk of homelessness appears increased among individuals most likely to come to the attention of the authorities during childhood (including placement for adoption or foster care). However, the involvement of outside agencies is likely to be an indicator of a history of adversity or of an exceptionally serious event that places individuals at risk. The pattern of associations between the indicators of childhood adversity and the other domains of life experiences considered in this study (mental illness, criminal behavior, and addiction problems) lends some support to this idea. The findings are consistent with the view that young people at the greatest risk of becoming homeless should, and probably could, be identified early, through schools, pediatricians' offices, or social service agencies ( 40 ).
Consistent with previous research, academic underachievement and early socioeconomic difficulty were significantly and independently related to homelessness ( 5 , 41 , 42 , 43 ). Economic hardship in childhood, including homelessness, may perpetuate and heighten the risk of homelessness later in life. Similarly, lack of educational qualifications will reduce the prospect of individuals' reintegrating into society and thereby increase risk of chronic homelessness. Along with the findings for indicators of childhood adversity, investment in prevention efforts should be directed toward factors that occur comparatively early in the life course that appear to predispose young people to episodes of homelessness.
After controlling for other factors, we found that a diagnosis of depression and receiving psychiatric care in the past five years were associated with homelessness. Research with homeless groups suggests that in most cases, psychopathology and substance abuse precede the onset of homelessness, supporting a view of mental disorders as risk factors for homelessness among young people, but it must be acknowledged that disorders can also follow a period of homelessness ( 8 , 14 , 42 , 44 , 45 ). Persons who have been or are currently homeless appear vulnerable to mental illness, yet the economic circumstances of these individuals are likely to obstruct their ability to access treatment. The development of a public health policy that facilitates access to treatment in a sustained way and in a variety of settings (such as shelters and community centers) is needed ( 46 ).
Drug use was independently associated with homelessness. Once a person becomes homeless, contact with other homeless people may increase the opportunities to obtain drugs, and drug use may serve as a means of coping with a very challenging lifestyle ( 47 ). Research suggests that there are bidirectional processes underlying the link between drug use and homelessness, such that the presence of one may predispose an individual to the other ( 24 , 47 ). Prospective, longitudinal research is therefore required to disentangle this possibility in a population-based sample. When assessed in the context of other hypothesized correlates, alcohol-related problems were not associated with homelessness. It is possible that by virtue of being a population-based sample (in which the definition of ever homeless included those who had been or were currently homeless) this study had a lower proportion of respondents with alcohol dependence than is typically included in studies of homeless people ( 11 , 12 , 48 ). On the other hand, recent work has found that drug abuse is more strongly associated than alcohol abuse with a first homeless episode, indicating that drug abuse may have become a more important risk factor for homelessness among young people in the United States ( 47 ).
Nonresponse is likely to have affected the pattern of derived results. Factors contributing to nonresponse included the respondent's being incarcerated, institutionalized, physically or mentally incapable, or untraceable ( www.cpc.unc.edu/projects/addhealth ). These factors may have produced an underrepresentation of respondents with dependence on drugs and alcohol, criminal backgrounds, mental health problems, and homelessness itself. The hidden and mobile nature of the homeless population means that their numbers and characteristics cannot be readily determined ( 5 ). The development of truly representative samples of homeless people, therefore, poses challenges that may be impossible to overcome. Nevertheless, replication of these findings with other population-based samples is needed.
Rates of conviction (or pleading guilty) in a juvenile (7%) or adult (15%) court were low in the sample with a history of homelessness compared with rates in some reports. Moreover, when assessed in the context of other correlates, involvement in crime (as victim or as perpetrator) was not significantly associated with homelessness. The association between criminality and problems with drugs (which remained a significant predictor) may account for this effect. This group of findings highlights the value of using population-based samples to examine the etiology of homelessness. Criminality and antisocial behavior, when assessed in conjunction with events occurring in childhood and with mental health problems, may not be of primary importance. With regard to the temporal relationship between crime and homelessness, it is interesting that a recent study of 14- to 25-year-olds found that criminal behavior followed, rather than preceded, homelessness ( 49 ).
Our study is based on cross-sectional data. Several of the variables pertinent to our work (indicators of child abuse and neglect, for example) were not assessed during adolescence (waves 1 and 2 of the Add Health study), and the assessment of homelessness did not include the date it was first experienced. This data set, therefore, did not allow us to test temporal relationships between risk factors and homelessness. An important direction for future research will be to include more detailed, dated information regarding housing and homelessness as part of prospective, population-based studies ( 17 ). A second limitation was a reliance on self-report and retrospective data collection about critical events occurring in childhood. However, respondents provided information knowingly for research purposes but were not informed of our hypotheses about associations between early childhood experiences and later experiences and events. This aspect of the design may have reduced the possibility of a reporting bias for this material. Research also shows that runaway and young homeless people are able to provide accurate accounts of childhood abuse and poor family functioning ( 39 ).
Conclusions
This study is among the first to investigate the role of hypothesized risk factors for homelessness in a nationally representative, population-based sample.
The findings indicate that experiences related to the separation of children from their parents or caregivers were associated with homelessness. Factors that reflect the provision of emotional and material support by parents (or lack thereof) were also associated with homelessness. Other domains that were linked to homelessness included socioeconomic disadvantage, indicators of mental illness, and problems with drugs. The results are consistent with previous research investigating the etiology of homelessness, yet this study advances understanding by considering the relative role of several factors thought to precede, accompany, or follow episodes of homelessness. Based as they are on a nationally representative U.S. sample, the findings provide important insights into the relative role of various life experiences and their relationship to homelessness, and they highlight the need to understand the temporal nature of these links. Closer attention to meeting the emotional and material needs of individuals identified in childhood as experiencing dysfunctional family relations may reduce the burden of social care for a homeless population.
Acknowledgments and disclosures
This research used data from Add Health, a program project designed by J. Richard Udry, Ph.D., Peter S. Bearman, Ph.D., and Kathleen Mullan Harris, Ph.D., and funded by grant P01-HD31921 from the National Institute of Child Health and Human Development, with cooperative funding from 17 other agencies. Special acknowledgment is due Ronald R. Rindfuss, Ph.D., and Barbara Entwisle, Ph.D., for assistance in the original design. Persons interested in obtaining data files from Add Health should contact Add Health, Carolina Population Center, 123 W. Franklin St., Chapel Hill, NC 27516-2524 ( [email protected] ).
The authors report no competing interests.
1. Homelessness in the United States and the Human Right to Housing. Washington, DC, National Law Center on Homelessness and Poverty, Jan 2004Google Scholar
2. Hawg S: Mental illness and mortality among homeless people. Acta Psychiatrica Scandinavica 103:81–82, 2001Google Scholar
3. Fountain J, Howes S: Home and Dry? Homelessness and Substance Use in London. London, Crisis, 2002Google Scholar
4. More Than a Roof: A Report Into Tackling Homelessness. London, Department of Transport, Local Government and the Regions, 2002Google Scholar
5. Fitzpatrick S, Kemp P, Klinker S: Single Homelessness: An Overview of Research in Britain. Bristol, United Kingdom, Policy Press, 2000Google Scholar
6. Barrow SM, Herman DB, Cordova P, et al: Mortality among homeless shelter residents in New York City. American Journal of Public Health 89:529–534, 1999Google Scholar
7. Connelly J, Crown J: Homelessness and Ill Health. London, Royal College of Physicians of London, 1994Google Scholar
8. Koegel P, Burnham MA, Farr RK: The prevalence of specific psychiatric disorders among homeless individuals in the inner city of Los Angeles. Archives of General Psychiatry 45:1085–1092, 1988Google Scholar
9. Zapf PA, Roesch R, Hart SD: An examination of the relationship of homelessness to mental disorder, criminal behaviour, and health care in a pre-trial jail population. Canadian Journal of Psychiatry 41:435–440, 1996Google Scholar
10. McNiel DE, Binder RL, Robinson JC: Incarceration associated with homelessness, mental disorder, and co-occurring substance abuse. Psychiatric Services 56:840–846, 2005Google Scholar
11. Fichter M, Quadflieg N: Alcoholism in homeless men in the mid-nineties: results from the Bavarian Public Health Study on homelessness. European Archives of Psychiatry and Clinical Neuroscience 249:34–44, 1999Google Scholar
12. Greifenhagen A, Fichter M: Mental illness in homeless women: an epidemiological study in Munich, Germany. European Archives of Psychiatry and Clinical Neuroscience 247:162–172, 1997Google Scholar
13. Reardon M, Burns AB, Preist R, et al: Alcohol use and other psychiatric disorders in the formerly homeless and never homeless: prevalence, age of onset, comorbidity, temporal sequencing, and service utilization. Substance Use and Misuse 38:601–644, 2003Google Scholar
14. Molnar BE, Shade SB, Kral AH, et al: Suicidal behaviour and sexual/physical abuse among street youth. Child Abuse and Neglect 25:137–148, 1998Google Scholar
15. Herman DB, Susser ES, Struening EL, et al: Adverse childhood experiences: are they risk factors for adult homelessness? American Journal of Public Health 87:249–255, 1997Google Scholar
16. Ryan KD, Kilmer RP, Cauce AM, et al: Psychological consequences of child maltreatment in homeless adolescents: untangling the unique effects of maltreatment and family environment. Child Abuse and Neglect 24:333–352, 2000Google Scholar
17. Koegel P, Memamid E, Burnham MA: Childhood risk factors for homelessness among homeless adults. American Journal of Public Health 85:1642–1649, 1995Google Scholar
18. Tyler KA, Cauce AM: Perpetrators of early physical and sexual abuse among homeless and runaway adolescents. Child Abuse and Neglect 26:1261–1274, 2002Google Scholar
19. Bebbington PE, Bhugra D, Brugha T, et al: Psychosis, victimisation and childhood disadvantage: evidence from the second British National Survey of Psychiatric Morbidity. British Journal of Psychiatry 185:220–226, 2004Google Scholar
20. Spauwen J, Krabbendam L, Lieb R, et al: Impact of psychological trauma on the development of psychotic symptoms: relationship with psychosis proneness. British Journal of Psychiatry 188:527–533, 2006Google Scholar
21. Herman DB, Susser ES, Struening EL: Childhood out-of-home care and current depressive symptoms among homeless adults. American Journal of Public Health 84:1849–1851, 1994Google Scholar
22. Greenberg GA, Rosenheck RA: Jail incarceration, homelessness, and mental health: a national study. Psychiatric Services 59:170–177, 2008Google Scholar
23. Randall G, Brown S: Prevention Is Better Than Cure: New Solutions to Street Homelessness From Crisis. London, Crisis, 1999Google Scholar
24. Johnson TP, Fendrich M: Homelessness and drug use: evidence from a community sample. American Journal of Preventive Medicine 32:S211–S218, 2007Google Scholar
25. Susser ES, Shang PL, Conover SA, et al: Childhood antecedents of homelessness in psychiatric patients. American Journal of Psychiatry 148:1026–1031, 1991Google Scholar
26. San Augustin M, Cohen P, Rubin D, et al: The Montefiore community children's project: a controlled study of cognitive and emotional problems of homeless mothers and children. Journal of Urban Health 76:39–50, 1999Google Scholar
27. Teesson M, Hodder T, Buhrich N: Substance use disorders among homeless people in inner Sydney. Social Psychiatry and Psychiatric Epidemiology 35:451–456, 2000Google Scholar
28. Caton CL, Dominguez B, Schanzer B, et al: Risk factors for long-term homelessness: findings from a longitudinal study of first-time homeless single adults. American Journal of Public Health 95:1753–1759, 2003Google Scholar
29. Fischer PJ, Breakey WR: The epidemiology of alcohol, drug, and mental disorders among homeless persons. American Psychologist 46:1115–1128, 1991Google Scholar
30. Resnick MD, Bearman PS, Blum RW, et al: Protecting adolescents from harm: findings from the National Longitudinal Study of Adolescent Health. JAMA 278:823–832, 1997Google Scholar
31. Harris KM, Florey F, Tabor J, et al: The National Longitudinal Study of Adolescent Health: Study Design. Available at www.cpc.unc.edu/projects/addhealth , 2003 Google Scholar
32. van den Bree MBM, Pickworth WB: Risk factors predicting changes in marijuana involvement in teenagers. Archives of General Psychiatry 62:311–319, 2005Google Scholar
33. La Gory M, Ritchey FJ, Mullis J: Depression among the homeless. Journal of Health and Social Behavior 31:87–102, 1990Google Scholar
34. Stiffman AR: Suicide attempts in runaway youths. Suicide and Life-Threatening Behavior 19:147–159, 1989Google Scholar
35. Unger JB, Kipke MD, Simon TR, et al: Homeless youths and young adults in Los Angeles: prevalence of mental health problems and the relationship between mental health and substance abuse disorders. American Journal of Community Psychology 25:371–394, 1997Google Scholar
36. Heffron WA, Skipper BJ, Lambert L: Risk factors for homelessness: a study of families of origin. Family Medicine 27:586–591, 1995Google Scholar
37. Susser E, Moore R, Link B: Risk factors for homelessness. American Journal of Epidemiology 15:546–556, 1993Google Scholar
38. Stata Statistical Software, Release 9. College Station, Tex, StataCorp, 2005Google Scholar
39. Whitbeck LB, Hoyt DR, Ackley KA: Families of homeless and runaway adolescents: a comparison of parent/caretaker and adolescent perspectives on parenting, family violence, and adolescent conduct. Child Abuse and Neglect 21:517–528, 1997Google Scholar
40. Bruegel I, Smith J: Taking Risks: An Analysis of the Risks of Homelessness for Young People in London. London, Peabody Trust, Safe in the City, 1999Google Scholar
41. Bonner AB: Social Exclusion and the Way Out: An Individual and Community Perspective on Social Dysfunction. Chichester, United Kingdom, Wiley, 2005Google Scholar
42. Eddins E: Characteristics, health status and service needs of sheltered homeless families. Journal of the Association of Black Nursing Faculty in Higher Education 4:40–44, 1993Google Scholar
43. Parks RW, Stevens RJ, Spence SA: A systematic review of cognition in homeless children and adolescents. Journal of the Royal Society of Medicine 100:46–50, 2007Google Scholar
44. North CS, Eyrich KM, Pollio DE, et al: Are rates of psychiatric disorders in the homeless population changing? American Journal of Public Health 94:103–108, 2004Google Scholar
45. Craig T, Hodson S: Homeless youth in London: I. childhood antecedents and psychiatric disorder. Psychological Medicine 28:1379–1388, 1998Google Scholar
46. O'Toole TP, Gibbon JL, Hanusa BH, et al: Self-reported changes in drug and alcohol use after becoming homeless. American Journal of Public Health 94:830–835, 2004Google Scholar
47. Johnson TP, Freels SA, Parsons JA, et al: Substance abuse and homelessness: social selection or social adaptation. Addiction 92:437–445, 1997Google Scholar
48. Farrell M, Howes S, Taylor C, et al: Substance misuse and psychiatric comorbidity: an overview of the OPCS National Psychiatric Morbidity Survey. International Review of Psychiatry 15:13–17, 2003Google Scholar
49. Martijn C, Sharpe L: Pathways to youth homelessness. Social Science and Medicine 62:1–12, 2006Google Scholar

