
Burnout in Nonhospital Psychiatric Residential Facilities
Burnout is a multidimensional syndrome involving the helping professions. It can affect the quality of services and compromise individuals' health. Burnout is associated with absenteeism, decreased job satisfaction, intention to quit the job, depression, anxiety, sleep disturbances, memory impairment, and physical complaints ( 1 , 2 ).
Burnout consists of three dimensions: emotional exhaustion, which refers to feelings of being overextended and depleted of one's emotional and physical resources; depersonalization, which is related to negative or excessively detached response toward clients of public services; and reduced sense of personal accomplishment, which concerns feelings of incompetence about job performance ( 3 ).
It has been reported that burnout, depression, and anxiety share several characteristics. However, empirical studies suggest that burnout and depression are separate nosological entities with independent courses ( 4 , 5 ). Burnout is not recorded in the section of mental and behavioral disorders (codes F00–F99) of the ICD-10 ( 6 ). It is included among factors influencing health status and contact with health services (codes Z00–Z99); indeed, it requires clinical attention because it can signal a decrease in level of personal functioning.
To prevent or reduce burnout it is important to assess and monitor the work environment because burnout can be triggered by stressful working conditions. Studies of mental health professionals have shown that associated working stressors include overload, time pressure, understaffing, negative social climate in the workplace, conflicts with patients, job insecurity, and organizational changes ( 7 ). At the same time, it has been recognized that job characteristics (including feedback about work performance, autonomy, and social support) influence job satisfaction and work engagement and may be associated with feelings of burnout ( 1 ).
Multicenter studies have shown that sources of stress differ between acute psychiatric care hospital wards and community-based mental health care ( 8 ) and that there are different burnout levels among mental health professionals according to the nation in which they work ( 9 ). Further research with specific samples in regard to profession, setting of care, and health care system is needed.
The purpose of this survey was to improve knowledge about the phenomenon of burnout among Italian mental health professionals who work in the setting of nonhospital psychiatric residential facilities. Such facilities have proliferated in Italy in the past three decades to promote psychosocial rehabilitation of patients with severe mental illness ( 10 ). Specifically, this study aimed to estimate levels of burnout and identify job risk factors for emotional exhaustion, depersonalization, and reduced sense of personal accomplishment.
Methods
This study is based on a convenience sample surveyed between May and September 2007. The research project was proposed to the service managers of 13 nonhospital psychiatric residential facilities of northern Italy. All agreed to participate and provided the staff lists of nurses, nurse assistants, and educators. A research assistant met with all 243 mental health professionals immediately before or after their work shift and asked each to complete a self-administered anonymous research questionnaire and return it to a collection box. A total of 202 workers gave informed consent and returned completed questionnaires, giving a response rate of 83%. Study procedures were approved by the local ethical committee.
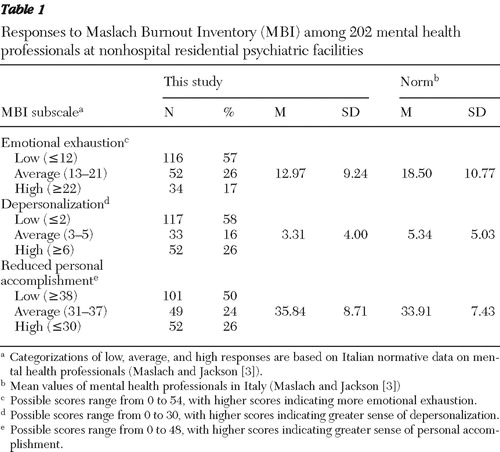
The research questionnaire was developed according to a literature review. Sociodemographic data included gender, age, marital status, children, profession, and education level. Burnout was assessed with the Maslach Burnout Inventory ( 11 ), which consists of three subscales, for emotional exhaustion, depersonalization, and personal accomplishment. For each item, possible scores range from 0 to 6, with higher scores indicating greatest frequency of feelings of burnout. According to the scoring instructions ( 3 ), burnout exists when the threshold for each subscale is reached (emotional exhaustion, ≥22; depersonalization, ≥6; and personal accomplishment, ≤30). Work-related aspects included duration of experience in mental health, job characteristics, correspondence of current job to one's own aspirations, workload, relationship with colleagues, and support from coordinators, who supervise the work of small teams of professionals.
Job characteristics were evaluated through the five subscales of the Job Diagnostic Survey ( 12 ): feedback about results (information about performance effectiveness), task significance, task variety, task identity (the degree to which one's job requires the completion of a specific piece of work with visible results), and autonomy. For each item, possible scores range from 1 to 7, with higher scores indicating the greatest extent to which the respondent's own job possesses the characteristic being assessed. For each subscale, it is possible both to calculate the mean of the items and also to sum the items; in the latter case possible scores range from 3 to 21. Low-level burnout was defined as scores under 15 ( 13 ).
Choosing one of the three response options for each item, participants evaluated the correspondence of the current job to their aspirations (not at all, partial, or complete), workload (excessive, regular, or suitable), relationships with colleagues (negative, neutral, or positive), and support from coordinators (poor, neutral, or strong).
Univariate logistic regressions were used to explore the association of burnout with sociodemographic variables as well as with work-related aspects. All variables that showed significant crude odds ratios (ORs) were included together in a multiple logistic regression to obtain adjusted odds ratios (AORs). The dependent variables were burnout dimensions, which were used as dichotomous variables (high versus low or average) referenced to Italian mental health norms ( 4 ). Differences in mean values were tested by a two-tailed t test or analysis of variance. Differences in frequency distributions were tested by the Mann-Whitney U test and Kruskal-Wallis test. A p value <.05 was considered statistically significant. Data analysis was performed with SPSS, version 13.0.
Results
Most of the 202 respondents were female (N=129, 64%), aged 35–44 years (N=98, 48%), and married (N=105, 52%); 124 (61%) had children living with them. They were nurses (N=62, 31%), nursing assistants (N=93, 46%), and educators (N=47, 23%) with a mean±SD of 12.07±3.19 years of education. They were employed in mental health services for 14.8±6.6 years.
The Job Diagnostic Survey scores were as follows: task variety, 4.31±1.31; task identity, 4.9±1.05; task significance, 3.94±1.16; autonomy, 4.15±1.06; and feedback about results, 4.75±1.09. The number of participants who had low scores on the Job Diagnostic Survey subscales were as follows: task significance, 142 (70%); autonomy, 139 (69%); skill variety, 109 (54%); feedback about results, 93 (46%); and task identity, 75 (37%).
Most of the respondents (N=115, 57%) stated that their current job corresponded to their aspirations. Considering workload, 104 (51%) participants defined it as regular, 66 (33%) defined it as suitable, and 27 (13%) defined it as excessive; five (3%) did not answer. Positive relationships with colleagues were reported by 123 (61%) participants, followed by 65 (32%) who reported neutral relationships with colleagues, and nine (4%) who reported negative relationships with colleagues; five (3%) did not answer. Seventy-eight (39%) participants reported having strong support from coordinators, 68 (34%) described support as neutral, and 47 (23%) reported it as poor; nine (4%) did not answer. Participants who responded that they had a suitable workload had significantly better scores on feedback about results, task identity, and support from coordinators (Mann-Whitney U test, respectively, 661.00, p=.005; 404.50, p≤.001; and 374.50, p≤.001).
Six (3%) participants reached the thresholds on all three Maslach Burnout Inventory subscales; 100 (50%) showed scores that reached the thresholds on one or two subscales; 96 (48%) had no score that reached the threshold ( Table 1 ). There was no significant difference between professional groups in mean values of emotional exhaustion, depersonalization, and sense of personal accomplishment.
 |
Univariate logistic regressions showed that emotional exhaustion was significantly associated with age (OR=.51, 95% confidence interval [CI]=.29–.89, p=.019), workload (OR=.41, CI=.23–.74, p=.003), support from coordinators (OR=.35, CI=.21–.60, p<.001), task variety (OR=2.86, CI=1.22–6.70, p=.016), task identity (OR=2.52, CI=1.17–5.40, p=.018), and feedback about results (OR=5.32, CI=2.18–12.95, p<.001). When these variables were entered together, only age, support from coordinators, and feedback about results were associated with emotional exhaustion ( Table 2 ). Considering the AORs, we found that the risk of high emotional exhaustion for those who reported low feedback about results was 4.4 times higher than the risk for those who reported high feedback about results (p=.008). Workers with poor support from coordinators were likelier to have emotional exhaustion than those with strong support (p=.007). Professionals aged 18–34 were more likely to have emotional exhaustion than those over age 45 (p=.034).
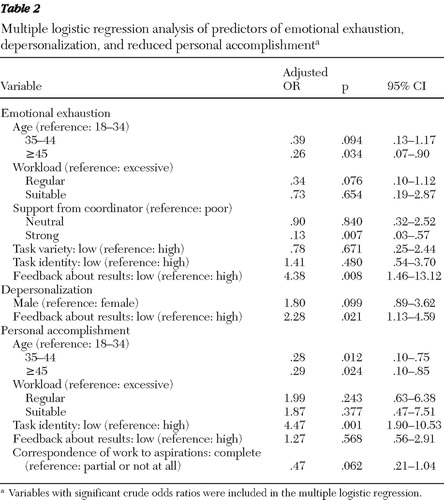 |
Univariate logistic regressions showed that depersonalization was somewhat associated with gender (OR=1.92, CI=.98–3.73, p=.056) and significantly associated with feedback about results (OR=2.12, CI=1.08–4.14, p=.029). When these variables were entered together, only feedback about results was associated with depersonalization ( Table 2 ). Considering the AORs, we found that participants with low feedback about results were 2.3 times likelier than those with high feedback scores to have feelings of depersonalization (p=.021).
Univariate logistic regressions showed that feelings of personal accomplishment were significantly associated with age (OR=.60, CI=.37–.97, p=.038), workload (OR=.58, CI=.35–.94, p=.028), feedback about results (OR=2.31, CI=1.18–4.51, p=.014), task identity (OR=4.38, CI=2.22–8.65, p<.001), and correspondence to aspirations (OR=.41, CI=.21–.79, p=.008). When these variables were entered together, only age and task identity were associated with feelings of personal accomplishment ( Table 2 ). Considering the AORs, we found that workers aged 18–34 were more likely to have reduced feelings of personal accomplishment than older workers (p=.024). The risk of reduced feelings of personal accomplishment for those who scored low on task identity was 4.5 times higher than for those who reported high task identity (p=.001).
Discussion
To our knowledge, this is the first study to evaluate the presence of burnout among professionals working in nonhospital psychiatric residential facilities for adult patients with severe mental illness. Our results indicate the intensity of burnout risk associated with specific work-related variables.
Half of the sample was at risk of developing burnout, which can be considered a syndrome, because burnout is a process in which the occurrence of one dimension, especially emotional exhaustion, precipitates the others ( 2 ). This process needs special attention because emotional exhaustion implies the presence of depressive symptoms ( 1 ) and persons with more severe forms of burnout have shown higher frequency of depressive disorders ( 5 ).
Consistent with previous studies conducted in other mental health settings ( 7 , 8 ), our study found high burnout in 3% of the sample (six workers). There were no differences between professional groups in mean scores of burnout and job characteristics. These results can be explained by considering that although the professionals who participated in this study all play different roles and have specific responsibilities, they also perform many similar tasks, support patients, help patients carry out daily activities, and spend similar amounts of time with patients.
We found that low feedback about results, low identity with tasks, and poor support from coordinators were the main work-related factors associated with burnout. The lack of these variables, categorized as job resources, could make employees indifferent and disengaged toward their work ( 1 ). Both feedback about results and task identity can influence the level of internal motivation, work engagement, and job satisfaction ( 12 ). Finally, social support is the most extensively studied resource, and there is strong evidence that lack of support is linked to burnout ( 2 ). These job characteristics were relevant in our sample, because psychosocial rehabilitation of patients with severe mental illness implies that results that are more long term than immediate and that providers are working in teams. Therefore, the nature of the work means that results are not immediately visible, and they are not closely related to one's specific activities. The communication among professionals daily and in routine meetings is important not only for contributing to achievement of therapeutic aims, but also to give workers the opportunity to receive feedback on performance and to link activities to global aims and promote participation in decision making.
In accordance with previous studies ( 1 , 7 ), which reported that burnout is not an automatic consequence of work pressure, we found that workload was not associated with burnout when other variables were taken into account. However, it is noteworthy that in our sample only 13% referred to their work as excessive and participants who referred to it as suitable had significantly better scores on feedback about results, task identity, and support from coordinators. Even if these features are considered, our results highlight that job characteristics, particularly relational aspects, play a crucial role in determining burnout.
Among individual factors, age is the strongest demographic variable associated with burnout ( 2 ), probably for the lack of strategies younger employees have developed to cope with work difficulties ( 7 ). In agreement with this hypothesis, we found that young age predicted high emotional exhaustion and reduced feelings of personal accomplishment.
It would be interesting to compare our results with those from other types of nonhospital psychiatric residential facilities, such as facilities for young patients; however, we did not find such studies in our literature review. A nationwide study conducted with Finnish physicians working within the field of psychiatry found no difference in frequency of severe burnout between psychiatrists, child psychiatrists, and other physicians ( 14 ). Specifically in regard to the type of patients treated, it has been found that nurses who work exclusively with patients with severe mental illness are more likely to have high levels of stress than those who have heterogeneous clients ( 15 ).
The limitations of this study need to be taken into account. Although a census was executed, the sample was not randomly selected. Therefore it cannot be considered representative of Italian nonhospital psychiatric residential facilities. Other limitations concern the small sample and the lack of investigation of other professional groups (such as psychiatrists and psychologists) employed in these nonhospital psychiatric residential facilities. Finally, the cross-sectional design of the study does not allow causal statements to be made about the findings.
Conclusions
The findings of this study contribute to existing knowledge about burnout among mental health professionals, extending it to employees in residential facilities. The risk of developing burnout syndrome was high in the sample, and work-related social aspects were shown to be strongly associated with burnout. Despite the limitations of the study, our results underline that the monitoring of the symptoms and the detection of associated variables constitute an essential step toward the promotion of preventive intervention. Initiatives focused on improving workplace relationships and enhancing job resources, such as feedback about results, task identity, and support from coordinators, appear necessary to reduce the risk of burnout syndrome.
Acknowledgments and disclosures
This study was supported by grant RC 2006/2008 from the Italian Ministry of Health.
The authors report no competing interests.
1. Demerouti E, Bakker AB, Nachreiner F, et al: A model of burnout and life satisfaction amongst nurses. Journal of Advanced Nursing 32:454–464, 2000Google Scholar
2. Maslach C, Schaeufeli WB, Leiter MP: Job burnout. Annual Review of Psychology 52:397–422, 2001Google Scholar
3. Maslach C, Jackson S (eds): MBI Maslach Burnout Inventory Manual [in Italian]. Florence, Italy, Organizzazioni Speciali, 1993Google Scholar
4. Sonnenshine M, Sorbi MJ, van Doornen LJP, et al: Evidence that impaired sleep recovery may complicate burnout improvement independently of depressive mood. Journal of Psychosomatic Research 62:487–494, 2007Google Scholar
5. Ahola K, Honkonen T, Kivimaki M, et al: The relationship between work-related burnout and depressive disorders: results from the Finnish Health 2000 Study. Journal of Affective Disorders 88:55–62, 2005Google Scholar
6. ICD-10 Classification of Mental and Behavioral Disorders: Diagnostic Criteria for Research. Geneva, World Health Organization, 1993Google Scholar
7. Kilfedder CJ, Power KG, Wells TJ: Burnout in psychiatric nursing. Journal of Advanced Nursing 34:383–396, 2001Google Scholar
8. Sorgaard KW, Ryan P, Hill R, et al: Sources of stress and burnout in acute psychiatric care: inpatient vs community staff. Social Psychiatry and Psychiatric Epidemiology 42:794–802, 2007Google Scholar
9. Reininghaus U, Priebe S: Assessing morale in community mental health professionals: a pooled analysis of data from four European countries. Social Psychiatry and Psychiatric Epidemiology 42:237–243, 2007Google Scholar
10. de Girolamo G, Picardi A, Santone G, et al: The severely mentally ill in residential facilities: a national survey in Italy. Psychological Medicine 34:1–11, 2005Google Scholar
11. Maslach C, Jackson S (eds): The Maslach Burnout Inventory Manual ("Human Services Survey"). Palo Alto, Calif, Consulting Psychologists Press, 1981Google Scholar
12. Hackman R, Oldham G: Development of the Job Diagnostic Survey. Journal of Applied Psychology 60:159–170, 1975Google Scholar
13. Maeran R, Martino G (eds): Job Diagnostic Survey. Instrument for Analysis of Job Satisfaction by Hackman and Oldham [in Italian]. Padova, Italy, Logos Edizioni, 1996Google Scholar
14. Korkeila JA, Tory S, Kumpulainen K, et al: Burnout and self-perceived health among Finnish psychiatrists and child psychiatrists: a national survey. Scandinavian Journal of Public Health 31:85–91, 2003Google Scholar
15. Edwards D, Burnard P, Coyle D, et al: A stepwise multivariate analysis of factors that contribute to stress for mental health nurses working in the community. Journal of Advanced Nursing 36:805–813, 2001Google Scholar

