
Rates of Unemployment and Incidence of Police-Initiated Examinations for Involuntary Hospitalization in Florida
Much scholarly literature focuses on the ethical and legal issues raised by coerced treatment of persons with mental illness whose behavior threatens the safety of others ( 1 , 2 ). A smaller, more empirical, body of literature describes attempts to estimate and predict the incidence of dangerous behavior in this population ( 3 , 4 ). Our analyses contribute to a third body of empirical work concerned with variation over time in society's tolerance for dangerous behavior exhibited by such persons ( 5 , 6 , 7 , 8 ). We believe that expanding and drawing attention to this literature could help persons better understand variation over time in the demand for their services and to plan accordingly.
Catalano and colleagues ( 8 ), drawing from work in social psychology ( 9 , 10 , 11 , 12 ), hypothesized that the likelihood of aggressive behavior increases in populations coping with contracting economies. They tested their arguments in San Francisco and Pittsburgh. Both tests supported the hypothesis that the number of men involuntarily admitted into treatment would increase when the labor market contracted ( 5 , 6 ). Results for women in San Francisco, but not in Pittsburgh, also supported the hypothesis.
These findings raise several important issues. First, the external validity of the San Francisco and Pittsburgh results remains unclear. Second, the two studies leave open the question of how much, if any, of the discovered associations arose not from an increase in the number of persons who threatened others but from reduced tolerance in the community for threatening behavior. Indeed, the theories invoked to justify these two studies support both mechanisms ( 8 , 9 ).
We address these limitations in the studies by Catalano and colleagues by replicating the tests in one of America's most diverse and populous states—Florida. The data from Florida allow us to improve upon the previous tests in two ways. First, we can determine if the citywide San Francisco and Pittsburgh findings generalize to a much larger state population observed more recently. Second, the Florida data allow us to estimate, as described below, the economy's effect on tolerance for—as opposed to the incidence of—dangerous behavior. Florida's records count persons who were involuntarily presented for involuntary psychiatric examination, as opposed to only those who were admitted. Florida's system also distinguishes between presentations for danger to others and for neglect or disability as well as between those initiated by mental health professionals and by law enforcement officials.
We hypothesized that the weekly incidence of involuntary psychiatric examinations initiated by law enforcement officials for harm to others varies positively with the number of persons who lose their jobs as a result of reduced demand for labor. Given the sex differences found between the San Francisco and Pittsburgh studies, we tested the hypothesis separately for men and women. Rejecting the null hypothesis would imply that reduced tolerance remains a plausible explanation for the association between economic contraction and involuntary psychiatric hospitalizations.
Circumstances other than reduced tolerance could induce an association over time between a contracting economy and involuntary psychiatric examinations for danger to others. As argued in the San Francisco and Pittsburgh studies, for example, a contracting economy may increase the number of persons with mental illness whose behavior threatens others. Indeed, we know from epidemiologic studies that contraction of labor markets predicts the number of undesirable job and financial events experienced by the population, especially the middle class ( 13 ). These events increase the risk of psychological distress, which increases the likelihood of using mental health services. Some fraction of this population in Florida with psychological distress resulting from these events may be involuntarily examined, which may induce the association for which we tested.
We attempted to control for this possibility by including as a covariate in our test equations the number of persons in Florida for whom mental health professionals sought involuntary hospitalization for danger to others. We reasoned that mental health professionals would be less influenced than police by intolerance in the community and more likely to seek hospitalization for persons who meet the criteria for commitment. We also reasoned that the community is more likely to contact the police than it is to contact mental health professionals after encountering persons who may be a danger to others ( 8 ); thus, even if the number or behavior of such persons is unchanged, the number of police-initiated involuntary hospitalizations will increase. We assumed that the argument for intolerance is strengthened if any association between economic contraction and police-initiated involuntary hospitalization for danger to others still exists after the analyses control for involuntary hospitalizations initiated by mental health professionals for danger to others.
Even with the above control, our explanation would remain vulnerable to the argument that a contracting economy reduces the population with sufficient insurance or income to seek help from mental health professionals. Without such help, some fraction of the newly unserved population becomes increasingly ill and meets the standard for involuntary examination, regardless of tolerance in the community. Because a mental health professional no longer sees these persons, the police instead present them for examination.
To control for this possibility we added the number of persons presented for examination by law enforcement for disability and neglect to our test equations. We can think of no reason why unmet need would induce behavior threatening to others but not disablement and neglect. Indeed, both circumstances often arise from substance use ( 14 ).
Methods
Data
Florida's nearly 17 million residents represent 5.8 percent of the U.S. population. The 1999 median household income of Floridians was $38,819, compared with $41,994 nationwide. Estimates from 1999 indicate that one-eighth of Floridians and of all U.S. citizens were living below the poverty line. A majority of Floridians are white (78.0 percent), 14.6 percent are black, and 1.7 percent are Asian. One-sixth (16.8 percent) is Hispanic ( 15 ).
Florida has centrally collected client-level data on involuntary psychiatric examinations since 1997. All facilities conducting such examinations are required by Florida statutes (F.S. section 394) to submit these data ( 16 ). Involuntary examinations may last up to 72 hours and require reason to believe that the person has a mental illness and is gravely disabled or will harm others or self if not treated. Examinations take place in receiving facilities designated by the Department of Children and Families that include psychiatric units of large hospitals, psychiatric hospitals, and inpatient units of community mental health centers. Examinations may be initiated by law enforcement officials or mental health professionals or by orders of a judge ( 17 ).
Various outcomes can result from involuntary examinations. Individuals may be released if they do not meet the criteria for both having a mental illness and having the potential to harm self, to harm others, or to be neglectful of self-care. Some individuals, if competent to do so, may agree to voluntary inpatient treatment, and others may be retained involuntarily for inpatient placement. Inpatient placement orders may be up to six months in length per order. Florida statute did not allow for involuntary outpatient placement during the study period.
We used the client-level data to create weekly counts of involuntary examinations based on evidence of mental illness and a likelihood of harm to others. We began our series with the week beginning Sunday, July 4, 1999. The series ended 208 weeks (four years) later on Saturday, June 28, 2003 (last available data at the time of the test). This series is long enough to ensure that we could identify seasonality as well as have more than sufficient power to detect effects of unemployment of the size expected from the San Francisco and Pittsburgh studies.
In 2004 we obtained the weekly counts of initial unemployment insurance claims in Florida from the U.S Department of Labor; the weekly counts covered the same period as the hospitalization data. Unemployment insurance is generally available to a worker if a job loss was from "no fault of [the worker's] own" ( 18 ). Claims do not include job losses from injuries or illness, for which workers' compensation and disability benefits are administered separately. Initial claims include only new applicants and therefore measure recent job losses.
Analyses
We first modeled presentations for examination by law enforcement (excluding judges) for danger to others as a function of presentations by law enforcement for disability and neglect and of presentations by mental health professionals for danger to others. We estimated separate models for men and women. We inspected the residuals of these models for autocorrelation unique to presentations by law enforcement for danger to others. We used the strategy devised by Dickey and Fuller ( 19 ) and by Box and Jenkins ( 20 ) to identify and model autocorrelation. The strategy of autoregressive, integrated, moving average (ARIMA) modeling draws from a very large family of models that describe autocorrelation in time series.
We then added monthly change (that is, first differences) in the unemployment insurance claims variable to the equation and specified the variable with no delay and a delay of one through three weeks to capture any delayed effects. We then estimated this final equation, inspected the residuals for autocorrelation, and if necessary, added any required Box-Jenkins parameters. We also deleted any parameters that did not reach significance at p<.05 (one-tailed test) and estimated the equation again.
The above steps yield the following general test equation.
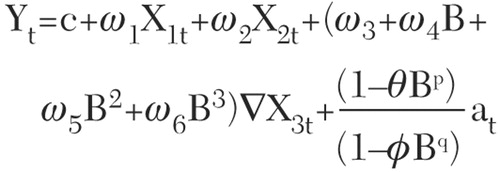
Y t is the number of men or women presented for examination by law enforcement officials for danger to others in Florida during week t; c is a constant. X 1t is the number of men or women presented for examination by mental health professionals for danger to others in Florida during week t. X 2t is the number of men or women presented for examination by law enforcement officials for disability and neglect in Florida during week t.
∇d indicates that the variable has been differenced at lag d (that is, value at week t subtracted from value at week t+d) to remove secular trends or cycles. X 3t is the number of initial claims for unemployment insurance compensation filed in Florida in week t. B n is the value of the variable at week t–n. Finally, ω0 to ω3 are effect parameters, θ is the moving average parameter, Φ is the autoregressive parameter, and a t is the error term at week t.
Results
The number of men presented by law enforcement officials for involuntary examination for harm to others in each of the 208 weeks beginning with the week beginning Sunday, July 4, 1999, totaled 5,896, with a mean±SD of 28.3±6.62 per week and a range of ten to 49 per week. The number of women totaled 3,079, with a mean of 14.8±4.68 per week and a range of six to 30 per week. The Dickey-Fuller test did not detect a secular trend in the series.
The number of initial unemployment insurance claims over the 208 weeks averaged 9,099±2,380 per week and ranged from 4,546 to 16,303 per week. The Dickey-Fuller test indicated that the series trended upward. We therefore "differenced" (that is, subtracted the value at week t from the value at week t+d) the series as indicated by the ∇X 3t parameter shown in the general test equation.
Table 1 shows the parameter estimates for men presented for examination by law enforcement officials for danger to others. Parameters for the initial model (that is, those controlling for autocorrelation as well as for presentations by mental health professionals for danger to others and by law enforcement officials for disability and neglect) and the final model are shown. As hypothesized, examinations moved positively over time with initial claims for unemployment compensation insurance. The association began in the week after changes in claims and continued through the third week after the change. Adding the unemployment claims variable to the equation controlling for autocorrelation and the two other categories of presentations increased R 2 variance from 25.8 to 33.3 percent.
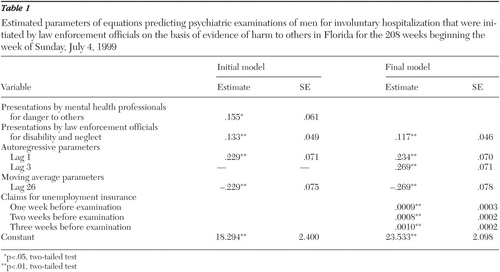 |
Consistent with results from the earlier test in San Francisco and Pittsburgh, men in Florida appeared to be at elevated risk of involuntary examination for involuntary hospitalization based on evidence of harm to others when initial claims for unemployment compensation increased. The claims increased in 88 of the 208 weeks tested. The sum of increased claims in those weeks was 114,567. The product of the sum of the three significant coefficients for claims from Table 1 (that is, .0008+.0009+ .0010=.0027) and the 114,567 job losses implies that, during times of job loss, law enforcement officials presented approximately 309 more men than expected on the basis of past presentation rates and the number presented for neglect by mental health professionals and by police.
Consistent with the Pittsburgh, but not San Francisco, findings, we found no association between economic contraction and coerced treatment of females.
We conducted two tests to estimate the likelihood that our findings resulted from analytic artifacts. First, we applied the routines developed by Chang and colleagues ( 21 ) to determine if outliers could have affected our results. Identifying and controlling outliers did not change the results of the tests. Second, we estimated the final models with the natural logarithm of all the dependent variables to test the possibility that variability over time in the variance of the series may have induced a type I error. The results remained the same with the obvious exception of the metric of the estimated parameters.
Other parameters in the initial model shown in Table 1 describe temporal variation in examinations of men initiated by law enforcement officials for danger to others. These examinations appear to have stronger "memory" than examinations initiated by mental health professionals for danger to others or by law enforcement officials for disability and neglect, in that after the analyses controlled for both, a high or low value of initiations by law enforcement officials appears, followed by similar, although attenuated, values in the next week. Examinations of men, moreover, exhibit an "echo" at 26 weeks such that unusually large or small numbers examined in a week predicts a similar, but decreasing, outlier six months later.
Discussion
We found that contraction of the Florida economy predicted increases in the number of men with mental illness coerced into treatment for danger to others. Our results cannot be attributed to trends, seasonality or other cycles, or any tendency of the involuntary examination time series to remain elevated or depressed after high or low values. Nor can the discovered association be attributed to any circumstance that would also affect presentations of men by mental health professionals for danger to others or presentations by law enforcement officials for disability and neglect. We also ensured that neither variability in variance nor outliers induced our findings. The fact that three tests in populations separated in space and time have yielded statistically significant associations for men suggests that chance alone cannot explain the connection.
Our finding of a 26-week "echo" for the number of examinations observed among men was unexpected. A post hoc explanation could be that men presented by law enforcement officials for danger to others are less likely to comply with treatment regimens than men presented by mental health professionals and, therefore, exhibit higher rates of relapse about six months after initial treatment ( 22 ).
We interpret our results as support for the argument that at least part of the association between economic contraction and coerced treatment of men for danger to others could be due to reduced tolerance for persons with mental illness. Our failure to detect a finding among women is consistent with the literature, which shows that women with mental illness are more likely to be tolerated ( 23 ).
We admit that we cannot directly measure tolerance with the data available to us. However, we do speculate that community tolerance is a reasonable explanation for our findings. Furthermore, the involuntary examination data from Florida permit a stronger test of the community tolerance hypothesis than was possible in San Francisco or Pittsburgh, because Florida's data included all persons who were presented for evaluation, not merely those who were admitted to involuntary hospitalization. The Florida data, therefore, better estimate the size of the population that the remainder of the community perceives to be dangerous to others.
We cannot rule out the possibility that something other than reduced tolerance induced the association we report. We suppose that mental health professionals could, in response to layoffs, reduce the number of persons they present for hospitalization, which would induce a relative increase in the number presented by police. Alternatively, layoffs could somehow induce an increase in the number of those at risk of presentation by the police but not by mental health professionals. Finally, presentations for disability may not completely capture changes in functioning associated with layoffs. Alternative explanations must exhibit no autocorrelation, including seasonality, secular trends, or the tendency to remain elevated or depressed after high or low values. Nor could the variable affect presentations of men either by police for disability or by mental health professionals for danger to others. The variable would, moreover, have to move synchronously with, but be otherwise unrelated to, weekly changes in the number of persons who lose their jobs as a result of reduced demand for labor.
We believe that our findings might help organizations that provide psychiatric services to persons with severe and persistent mental illness. Few obvious interventions exist to make community tolerance less sensitive to changes in employment, but systems can be prepared to anticipate and ameliorate the effect of layoffs on persons at risk of involuntary hospitalization. For example, the behavior of labor markets has been well studied, and methods for predicting near-term employment changes appear widely available to public and private agencies interested in the performance of local economies. It seems reasonable to explore how these methods might be combined with analyses such as those described in this article to allow providers to anticipate better the need for psychiatric services and prepare communities for more involuntary examinations. Our findings suggest, for example, that contracting economies may signal the need for greater capacity to treat persons with chronic illness brought into the system through civil commitment. Contracting economies may not, however, indicate the need for greater prevention efforts intended to reduce new incidence of violent behavior among persons with severe and persistent mental illness. Such prevention efforts may be better allocated to persons known, through unemployment compensation insurance agencies, to have lost jobs ( 12 ).
Further research should also establish whether the processes we describe affect the reporting of other events important to the providers of psychiatric services. Community tolerance for domestic violence ( 24 , 25 ), for example, might be measured through changes in bystander-initiated police reports of such events after adjusting for victim-initiated reports. Downturns in the labor market may induce disproportionate job losses among persons with stigma-carrying physical illnesses as well. For example, tests similar to those described in this article could examine labor market discrimination against persons with HIV infection.
Conclusions
Data from Florida converge with those from earlier but smaller studies to suggest that contracting economies are associated with an increase in the number of men with mental illness coerced into treatment because of a threat of danger to others. We speculate that this response reflects reduced community tolerance for dangerous behavior exhibited by men with mental illness. These findings imply that providers of psychiatric services could work with public and private employment agencies to develop models that predict demand for coerced treatment. The work also suggests that, during times of economic contraction, the mental health community might consider interventions to mitigate the effects of reduced tolerance toward persons with mental illness. For example, persons with mental illness who are at greater risk of detection in public and by the police might benefit from proactive diversion into preventive mental health treatment than from involuntary hospitalization.
Acknowledgments
Portions of data collection on involuntary hospitalizations were funded by grant R-01-MH-060217 from the National Institute of Mental Health and contract MO-308 with the Florida Agency for Health Care Administration.
1. Applebaum P: Almost a Revolution: Mental Health Law and the Limits of Change. New York, Oxford University Press, 1994Google Scholar
2. Monahan J, Lidz C, Hoge S, et al: Coercion in the provision of mental health services: the MacArthur studies, in Research in Community and Mental Health, Vol 10: Coercion in Mental Health Services. Edited by Morrissey J, Monahan J. Stamford, Conn, JAI, 1999Google Scholar
3. Monahan J, Steadman HJ, Silver E, et al: Rethinking Risk Assessment: The MacArthur Study of Mental Disorder and Violence. New York, Oxford University Press, 2001Google Scholar
4. Parry J, Hominik D, Skoler GD, et al: National Benchbook on Psychiatric and Psychological Evidence and Testimony. Washington, DC, American Bar Association, 1998Google Scholar
5. Catalano R, Novaco RW, McConnell W: A model of the net effect of job loss on violence. Journal of Personality and Social Psychology 72:1440-1447, 1997Google Scholar
6. Catalano R, Novaco RW, McConnell W: Layoffs and violence revisited. Aggressive Behavior 28:233-247, 2002Google Scholar
7. Catalano R, McConnell W, Forster P, et al: Psychiatric emergency services and the system of care. Psychiatric Services 54:351-355, 2003Google Scholar
8. Catalano RA, Kessell ER, McConnell W, et al: Psychiatric emergencies after the terrorist attacks of September 11, 2001. Psychiatric Services 55:163-166, 2004Google Scholar
9. Berkowitz L: Frustration-aggression hypothesis: examination and reformulation. Psychological Bulletin 106:59-73, 1989Google Scholar
10. Dollard J, Doob L, Miller N, et al: Frustration and Aggression. New Haven, Conn, Yale University Press, 1939Google Scholar
11. Folger R: Reactions to mistreatment at work, in Social Psychology in Organizations: Advances in Theory and Research. Edited by Murnighan K. Engelwood Cliffs, NJ, Prentice Hall, 1993Google Scholar
12. Vinokur AD, Price RH, Caplan RD: Hard times and hurtful partners: how financial strain affects depression and relationship satisfaction of unemployed persons and their spouses. Journal of Personality and Social Psychology 71:166-179, 1996Google Scholar
13. Dooley D, Catalano R: Why the economy predicts help-seeking: a test of competing explanations. Journal of Health and Social Behavior 25:160-176, 1984Google Scholar
14. Swartz MS, Swanson JW, Hiday VA, et al: Violence and severe mental illness: the effects of substance abuse and nonadherence to medication. American Journal of Psychiatry 155:226-231, 1998Google Scholar
15. United States Census Bureau: Florida Quickfacts, 2004. Available at http://quickfacts.census.gov/qfd/states/12000.htmlGoogle Scholar
16. McGaha A, Stiles PG, Petrila J: Emergency involuntary psychiatric examinations in Florida. Psychiatric Services 53:1171-1172, 2002Google Scholar
17. Christy A, Stiles P: The Florida Mental Health Act (The Baker Act): 2003 Annual Report. Tampa, University of South Florida, Louis de la Parte Florida Mental Health Institute, 2005Google Scholar
18. Unemployment Insurance Weekly Claims Data, Employment and Training Administration, United States Department of Labor, 2004. Available at http://workforcesecurity.doleta.gov/unemploy/claims.aspGoogle Scholar
19. Dickey D, Fuller W: Distribution of the estimators for autoregressive time series with a unit root. Journal of the American Statistical Society 74:427-431, 1979Google Scholar
20. Box G, Jenkins G, Reinsel G: Time Series Analysis: Forecasting and Control. London, Prentice Hall, 1994Google Scholar
21. Chang I, Tiao G, Chen C: Estimation of time series parameters in the presence of outliers. Technometrics 30:193-204, 1988Google Scholar
22. Miner CR, Rosenthal RN, Hellerstein DJ, et al: Prediction of compliance with outpatient referral in patients with schizophrenia and psychoactive substance use disorders. Archives of General Psychiatry 54:691-694, 1997Google Scholar
23. Schnittker J: Gender and reactions to psychological problems: an examination of social tolerance and perceived dangerousness. Journal of Health and Social Behavior 41:224-240, 2000Google Scholar
24. Catalano R, Lind S, Rosenblatt A, et al: Unemployment and foster home placements: estimating the net effect of provocation and inhibition. American Journal of Public Health 89:851-856, 1999Google Scholar
25. Catalano R, Lind S, Rosenblatt A, et al: Economic antecedents of foster care. American Journal of Community Psychology 32:47-56, 2003Google Scholar

