
The Capacity to Vote of Persons With Serious Mental Illness
In a democratic society, the right to vote is one of the most valued civil rights, because it is considered essential to the protection of other rights. At the founding of the United States this right was limited to a minority of the population; however, in the past two centuries, the general trend has moved toward universal suffrage ( 1 ). There are, however, groups that are still often denied access to the ballot, including persons with mental illness ( 2 , 3 ).
States in this country generally have the authority to determine standards of competence to vote and to exclude persons they deem not capable of voting. Most states have established criteria in constitutional provisions, statutes, or regulation by which some of those with mental disabilities are denied the franchise ( 3 ). However, there are at least two problems with most of these criteria. First, the wording is often archaic and vague (for example, denying suffrage to any "idiot" or "insane person"), and little guidance is provided for determining the meaning of these terms. Second, the criteria often are based on diagnosis, general incompetence, or membership in a class (for example, all persons under guardianship by reason of mental disability) rather than on an assessment of the functional abilities that are relevant to the act of voting ( 4 ). Therefore, these criteria may be overbroad and may inappropriately disenfranchise potentially competent voters. Under contemporary principles of mental health law and ethics, persons' freedom to make their own decisions should be denied only on the basis of an assessment of their specific and relevant functional capacities ( 5 ). Because voting is an important right in a democracy, it should not be denied under any broader standard of incompetence than is necessary ( 6 , 7 ).
Yet the right to vote of persons with mental illness remains a subject of controversy, with policy makers and members of the general public often appearing to hold the view that serious mental illnesses per se render persons incompetent to vote. Voters in Maine, for example, twice refused to replace a constitutional provision that denied the franchise to all persons under guardianship because of mental disabilities ( 8 , 9 ), although voters in New Jersey recently approved the amendment of a similar provision ( 10 ). Missouri officials defended their state's constitutional restrictions on voting by persons under guardianship for mental disabilities against a challenge in federal court; the provision was upheld by an appeals court but only because it was interpreted as requiring individualized assessments of voting capacity ( 11 ). Rhode Island voting officials attempted to restrict voting by two persons found not guilty by reason of insanity—arguing in part that if they lacked responsibility for their criminal behavior, they could not be competent to vote—and vowed to challenge an administrative rejection of their position in court ( 12 ).
Despite this legacy of discrimination against persons with mental illness, the clear trend has been toward individualized determinations of mental capacity to vote. This approach, however, requires a functional standard of capacity and a method of applying it. One such standard was established in a 2001 federal district court decision in Maine, Doe v. Rowe, which struck down the provision in Maine's constitution that voters had twice refused to alter. In its opinion, the court adopted a narrow and specific test: persons are considered incompetent to vote only if they "lack the capacity to understand the nature and effect of voting such that they cannot make an individual choice ( 13 )." In addition to being well defined and straightforward to implement, this standard is both functionally related to the process of voting and narrow enough that it can limit the number of persons unnecessarily excluded from voting. (We use " Doe standard" to refer to these criteria.)
In a previous study, Appelbaum and colleagues ( 14 ) developed an instrument (the Competency Assessment Tool for Voting, or CAT-V) in which this standard was operationalized in a three-item questionnaire along with three additional items addressing appreciation of and reasoning about voting choices for comparative purposes. The CAT-V was then tested with 33 patients with very mild to severe Alzheimer's disease, and scores were found to correlate strongly with severity of dementia, suggesting construct validity. Furthermore, the CAT-V was easy and efficient to administer, taking less than four minutes, and had high interrater reliability.
In this study, we used the CAT-V to examine the consequences of applying the Doe standard to a population of community-dwelling individuals with serious mental illness and to examine the relationships of the measures in the CAT-V to established measures of mental illness severity and cognition. Our hypotheses were that most community-dwelling persons with serious mental illness would demonstrate good performance on this measure of voting capacity and that performance on the CAT-V would correlate inversely with cognition and, to a lesser degree, with mental illness severity.
Methods
Participants
A total of 52 participants were recruited from two clinics of the Washington Heights Community Service at the New York State Psychiatric Institute. The clinics provide services for community-dwelling patients with serious mental illness. Participants were recruited from both outpatient and day treatment services. Most attendees at the clinics are Hispanic (80%) (almost all are of Dominican descent), and the rest are African American (10%), white (5%), or of other races and ethnicities (5%). Participants had to be eligible to vote in New York State (over 18 and U.S. citizens), to be able to communicate in English, and to report that they would vote in English. Case managers approached patients about the study, and if they agreed to participate, the case managers referred them to a member of the research team in the clinic that day. Because case managers had the initial discussion with potential participants about enrolling in the study, we were not able to ascertain the number who refused to participate at that stage. However, eight of 60 potential participants (13%) declined to participate after speaking with the interviewer.
Assessment tools
We used the CAT-V instrument to assess capacity to vote ( 14 ). After an introduction that asks the respondent to imagine that it is Election Day for the office of governor, the interviewer inquires about the person's understanding of the nature and effect of voting, then reads aloud a description of two candidates and asks the person to choose one of them. Respondents are then asked to compare the candidates and identify ways that their choice could affect their own lives. Finally, they are asked to explain why they would or would not want to vote in the next election for governor.
The CAT-V is based on the structure and scoring criteria of other capacity assessment instruments and uses six questions to assess a person's performance on all four standard decision-making abilities: understanding, choice, reasoning, and appreciation. Each question is scored on a 3-point scale, where a score of 2 describes adequate performance on the measure, 1 marginal performance, and 0 clearly inadequate performance. The three questions used to assess understanding and choice were designed on the basis of the Doe standard for voting capacity. [A copy of the CAT-V is available as an online supplement to this article at ps.psychiatryonline.org .]
In addition, a voting simulation instrument was used to assess participants' abilities to perform the final step of voting: indicating a choice on a ballot. After administering the CAT-V questions, the interviewer gave the participant a simple ballot showing two boxes with a name beside each box and instructions on how to vote. The interviewer asked the participant to vote for one of the candidates on the ballot. This instrument was scored with a 3-point scale similar to that used for each item on the CAT-V. [The voting simulation instrument and its scoring criteria are presented in an appendix available as an online supplement to this article at ps.psychiatryonline.org .]
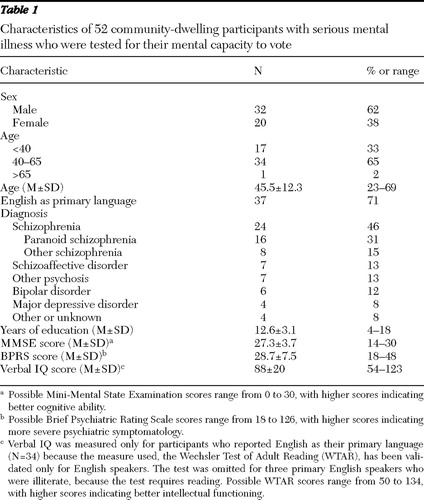
The other instruments used were the Mini-Mental State Examination (MMSE) ( 15 ) to measure overall cognition, an anchored 18-item version of the Brief Psychiatric Rating Scale (BPRS) to assess severity of the symptoms of mental illness ( 16 ), and the Wechsler Test of Adult Reading (WTAR) to approximate verbal IQ ( 17 ). The WTAR was omitted for participants who indicated that English was not their primary language, because it is not validated for that group.
Data gathering
Each respondent participated in a face-to-face interview with a medical student interviewer (RR), and all interviews were digitally recorded. Before the beginning of the study, the interviewer was trained by an investigator (PSA) experienced in administering the CAT-V, BPRS, and WTAR who also monitored the first ten interviews and scored them with the interviewer. The remaining interviews were scored by the interviewer. Items that the interviewer considered difficult to score were reviewed and scored jointly, based on review of the verbatim responses, audiotapes, or both. Participants' demographic data were obtained during the interview, and diagnoses were recorded from their charts. All data were gathered between November 1, 2007, and May 15, 2008.
Data analyses
For each participant, we created a Doe score (range 0–6) by summing the scores for understanding the nature and the effect of voting and for making a choice. A reasoning score (range 0–4) was created by summing the scores for the two reasoning questions, and the score on the remaining question constituted an appreciation score (range 0–2). Appropriate summary statistics and cross-tabulations displayed the patterns of participants' performance. Spearman's correlation coefficient and the Kruskal-Wallis chi square test were used to examine associations among the CAT-V measures and between performance on the voting capacity instruments and the scores on the MMSE, BPRS, and verbal IQ. Every fifth CAT-V interview (N=10) was rescored by a second scorer (PSA) to assess interrater reliability. Because of observed ceiling effects, percentage agreement, rather than the kappa statistic, was used as the statistic of reliability.
Human subjects protections
If a patient agreed to an interview, the interviewer described the nature of the study in detail and then verbally confirmed the eligibility criteria. All participants were assured that the information would be used for research purposes only, and they provided written informed consent. This study was approved by the institutional review board of the New York State Psychiatric Institute.
Results
Participant characteristics
Fifty-two participants completed the interview ( Table 1 ). Seventy-two percent of the sample had psychotic disorders, and another 20% had major mood disorders. Overall, severity of symptoms was consistent with a seriously ill outpatient population. Compared with the clinic population as a whole, males were somewhat overrepresented in the sample (62% vs. 50%), but the diagnostic and age distributions were representative of the clinic population.
 |
Performance on the CAT-V
The participants took a mean±SD of 4.3±1.9 minutes (range=2.3–9.2) to complete the Doe -standard questions and took 7.8±3.5 minutes (range=3.0–14.8) to complete the entire CAT-V interview. The scoring criteria showed good interrater reliability on most questions, as measured by percentage agreement: understanding nature of voting, 90%; understanding effect of voting, 80%; choice, 100%; comparative reasoning, 100%; consequential reasoning, 60%; and appreciation, 70%. Of the 30 Doe -standard responses used in the interrater reliability assessment, the raters agreed on 27 items (90%), and the disagreements on the remaining three items were by 1 point each.
The distribution of participants' scores on each of the CAT-V questions is shown in Table 2 . Most participants performed well on the Doe -standard questions, with a minimum of 90% (N=47) of participants obtaining the highest score on each Doe -related question and 92% scoring at least 5 out of 6 possible points on the Doe -standard total score. They performed equally well when asked to articulate a reason for preferring one candidate to another (comparative reasoning) but had more trouble describing the impact of their choices on their own lives (generating-consequences item; 77% scored the high score of 2).
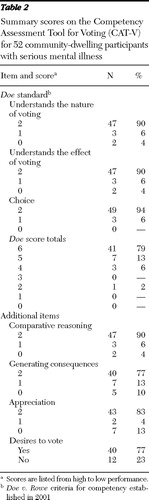 |
Comparisons of scores on the Doe questions with the reasoning and appreciation measures showed that the Doe scores correlated with ability to reason about voting (r s =.65, N=52, p<.001) but not with the ability to appreciate the effect of voting. Forty participants indicated that they wanted to vote in the next election for governor, and 12 said they did not. A desire to vote was not associated with scores on the Doe standard, the appreciation and reasoning questions, age, or years of education.
Performance on the voting simulation
Fifty-one participants completed the voting simulation. A total of 39 participants (76%) achieved the high score of 2. Only four participants (8%) received a score of 0. Of these, three had difficulty understanding the directions and therefore left the ballot blank; only one marked the wrong candidate. The participants who performed marginally (N=8, 16%) indicated the correct choice but in an incorrect fashion (with a check mark rather than the required X).
Relationships between performance and participant characteristics
With one exception, there were no significant correlations between the CAT-V questions or the desire to vote and scores on the MMSE, the BPRS, or verbal IQ. Higher scores on the reasoning questions of the CAT-V were associated with higher MMSE scores (r s =.48, N=47, p<.001). All but one of the participants who scored 22 or higher on the MMSE (with a top possible score of 30) also scored 3 or more on reasoning. This finding is consistent with the results found with Alzheimer's patients ( 14 ). The CAT-V scores were not associated with participants' age or education, except that participants who scored 2 on the generating-consequences item had more years of education than those who scored 0 or 1 (ranked-sum test: z=3.1, p=.002).
High scores on the voting simulation were associated with higher reasoning scores (Kruskal-Wallis χ2 =7.1, df=2, p=.029) but not with any other CAT-V measures or with scores on the MMSE, BPRS, or verbal IQ.
Discussion
This is the first known study to gather data on the competence to vote of community dwellers with mental illness and on the association of that competence with the severity of mental illness and other relevant variables. It demonstrates that in a sample of individuals with serious mental illness, a large majority understood the nature and effect of voting and could choose between two candidates. Only four participants received a score of less than 5 out of 6 on the group of questions that operationalize the standard established by the U.S. Federal District Court in Doe v. Rowe .
As in the previous study with Alzheimer's patients ( 14 ), Doe -related scores in this sample were not correlated with any demographic variables, including age and education level. In contrast to the Alzheimer's group, however, the scores of our sample were also not significantly correlated with cognition. This result may be due to the narrow distribution of Doe scores and comparatively higher cognitive scores of the patients in this study. In the Alzheimer's study, the subset of patients with higher MMSE scores (those with mild and very mild dementia, as defined by an MMSE score >19) also did not show as strong a correlation between Doe scores and cognitive capacity. Further, the Doe scores in that subset and in our sample were both almost uniformly high.
The Doe voting capacity standard is intended to be restrictive enough to protect the integrity of the vote yet permissive enough that it does not arbitrarily and unnecessarily deprive individuals of their rights. When compared with the more lenient procedure of allowing anyone with a desire to vote to do so, the Doe standard ensures that those who cast ballots have a basic understanding of the process in which they are engaging. In our sample, although most received the highest Doe -standard total score of 6 points, most of those who scored 5 or below expressed a desire to vote, indicating that not all who desired to vote had a complete understanding of the nature and effect of voting.
Although not included in the Doe v. Rowe opinion, the additional reasoning and appreciation questions were included in this study to clarify the implications of the Doe -standard criteria and to compare them with an alternative. The results indicate that most individuals with serious mental illness could reason about and appreciate the significance of voting and that participants' scores on the Doe criteria had a correlation with ability to reason about the consequences of a choice of candidates. However, they also indicate that including reasoning and appreciation in the criteria of voting capacity would have disenfranchised some would-be voters who met the Doe criteria—an unfortunate outcome. Further advantages of using the Doe criteria are the high interrater reliabilities and the ease and efficiency of administering the relevant questions, which took an average of less than five minutes to complete.
The necessity for including a choice item in the competence assessment can be questioned on the grounds that this portion of the capacity standard is assessed by implication at the time of voting. Anyone unable to make a choice would not be able to cast a ballot. In our sample, the three participants who did not make a choice wavered between the candidates and indicated that they would like more time or information. It is unclear whether they would have been equally unable to make a choice at the time of an actual election, because more time and information are usually available to decide about a candidate for a major office than were available in our interview. Therefore, our data seem to support omitting this question from the standard unless its inclusion can be shown to save time and avoid difficulties associated with assisting persons in getting to the polls or completing absentee ballots.
The right to vote is an important civil right, and in the absence of an indication of incapacity, a person should be assumed to be capable of voting. A large majority of our sample received high Doe scores; on the basis of these data, this assumption in general appears to be appropriate even for people with a severe mental illness. Therefore, we do not recommend that the relevant sections of the CAT-V be used as a general screening instrument for all persons with mental illness but that they be reserved for individuals whose voting capacity is in question (for example, during guardianship proceedings). Because Doe scores did not correlate with clinical measures, our data do not support the use of clinical criteria in the assessment of voting capacity.
The limitations of this study primarily concern the sample, which was not representative of persons with mental illness in general because it was not drawn randomly from that population and included only the more serious diagnoses. Moreover, many members of our sample, although now U.S. citizens, were foreign born. However, this chronically ill patient population, with a high prevalence of psychosis and with many individuals who required day treatment services, performed generally quite well. This outcome suggests that voting capacity in the outpatient population with mental illness may be even higher on average than in this study's sample. Additional research would be needed to address the possibility that more acutely ill or psychiatrically impaired samples might do worse, although the lack of correlation between performance and the severity of psychiatric symptoms in this sample is reassuring.
In the movement toward individualized determinations of mental capacity to vote, functional criteria such as those measured by the CAT-V can help to ensure that the standard for voting is relevant and appropriate. If the Doe -standard questions of the CAT-V are to be used for this purpose, then a judgment will have to be made about which scores represent adequate voting capacity. Although 6 correct out of 6 possible is clearly adequate, it is unclear whether 5 or 4 correct out of 6 should be acceptable as well. Our data alone are not sufficient to answer this question. However, to promote equal protection under the law, the criteria chosen for persons with a mental illness should not be more stringent than the standard applied to the general population. Therefore, we recommend that data on performance of individuals without a mental illness be used in establishing appropriate cutoffs for determining mental capacity to vote.
Conclusions
On the assumption that the high scores in this sample are confirmed in other groups of persons with serious mental illness, it may be appropriate to assume that as a group, persons with serious mental illness do not manifest a substantial incidence of incapacity to vote. This calls into question the legitimacy of criteria embedded in state constitutions, statutes, and regulations, as well as ad hoc efforts that would limit persons with serious mental illness from accessing the polls. Efforts to eliminate restrictive criteria and confine disqualification to the small number of persons who demonstrate functional impairment on voting-related criteria should enhance the democratic process while simultaneously protecting the integrity of the franchise.
Acknowledgments and disclosures
The authors report no competing interests.
1. Keyssar A: The Right to Vote: The Contested History of Democracy in the United States. New York, Basic Books, 2000Google Scholar
2. Shriner K, Ochs LA, Shields TG: The last suffrage movement: voting rights for persons with cognitive and emotional disabilities. Publius 27:75–96, 1997Google Scholar
3. Belluck P: States face decisions on who is mentally fit to vote. New York Times, June 17, 2007, p A-1Google Scholar
4. Hurme SB, Appelbaum PS: Defining and assessing capacity to vote: the effect of mental impairment on the rights of voters. McGeorge Law Review 38:931–1014, 2007Google Scholar
5. Moye J: Guardianship and conservatorship, in Evaluating Competencies. Edited by Grisso T, Borum R, Edens JF, et al. New York, Kluwer Academic, 2002Google Scholar
6. Karlawish JH, Bonnie RJ, Appelbaum PS, et al: Addressing the ethical, legal, and social issues raised by voting by persons with dementia. JAMA 292:1345–1350, 2004Google Scholar
7. Karlan PS: Framing the voting rights claims of cognitively impaired individuals. McGeorge Law Review 38:917–930, 2007Google Scholar
8. Kupersanin E: Judge restores voting rights to mentally ill in Maine. Psychiatric News 36:24, 2001Google Scholar
9. Appelbaum PS: "I vote. I count": mental disability and the right to vote. Psychiatric Services 51:849–850, 863, 2000Google Scholar
10. Livio SK: Two of four ballot questions defeated. Star Ledger, Nov 7, 2007, p 9Google Scholar
11. Missouri Protection and Advocacy Services v Carnahan, 499 F 3d 803 (8th Cir 2007)Google Scholar
12. Zezima K: 2 men long confined as insane regain their right to vote. New York Times, May 30, 2008Google Scholar
13. Doe v Rowe, 156 F Supp 2d 35 (D Me 2001)Google Scholar
14. Appelbaum PS, Bonnie RJ, Karlawish JH: The capacity to vote of persons with Alzheimer's disease. American Journal of Psychiatry 162:2094–2100, 2005Google Scholar
15. Folstein MF, Folstein SE, McHugh PR: "Mini-Mental State": a practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 12:189–198, 1975Google Scholar
16. Overall JE, Gorham DR: The Brief Psychiatric Rating Scale (BPRS): recent developments in ascertainment and scaling. Psychopharmacology Bulletin 24:97–99, 1988Google Scholar
17. Wechsler Test of Adult Reading. San Antonio, Tex, Psychological Corp, 2001Google Scholar

