
Disparities in Adequate Mental Health Care for Past-Year Major Depressive Episodes Among Caucasian and Hispanic Youths
The advent of the community mental health centers program in 1963 has led to a shift away from inpatient treatment in favor of community-based services for individuals affected by serious mental illnesses ( 1 , 2 ). More important, recent findings indicate a continued overall trend toward greater use of outpatient mental health care that now accounts for more than 59% of the nearly $12 billion spent in the United States to treat youths affected with mental disorders ( 3 ). Despite outreach efforts to treat these youths, a large proportion does not receive needed care, and there is particular concern about disparities in access to care across racial and ethnic groups ( 4 , 5 ). Indeed, studies demonstrate that Hispanic youths are less likely than Caucasian youths to receive specialty mental health services ( 6 , 7 , 8 , 9 ). Even when youths received treatment for mental health problems, Hispanics made fewer visits than Caucasians ( 10 , 11 , 12 ). An important area that has not been comprehensively investigated is whether these disparities exist in receiving a minimum of "adequate mental health care" for past-year major depressive episodes.
Following recent concerns about the levels of treatment received by individuals affected by serious mental illnesses, significant efforts have been made to ensure that mental health treatment is concordant with evidence-based guidelines ( 13 , 14 , 15 , 16 ). With the increasing involvement of primary care physicians in providing mental health care, the Agency for Healthcare Research and Quality developed evidence-based guidelines for the treatment of depression in primary care settings ( 17 ). The American Psychiatric Association also developed guidelines for the treatment of depression in specialty mental health settings ( 18 , 19 ). On the basis of these guidelines, a working definition of a minimum of "adequate mental health care" was defined in the literature as follows: either receipt of a prescribed medication in combination with four or more visits to a psychiatrist, psychologist, general medical doctor, or other medical doctor or if the individual is not psychotic, receipt of at least eight visits with a mental health specialist ( 20 , 21 ). Using this definition, we investigated racial and ethnic disparities in receiving adequate mental health care between Caucasian and Hispanic youths affected by past-year major depressive episodes. The topic is of keen importance because lack of adequate mental health care among youths represents a lost opportunity to intervene and possibly to prevent persistence of psychopathology into adulthood ( 22 ).
This study's framework draws from a well-validated theoretical model, Andersen's social behavioral model, which has been used to analyze mental health service use ( 23 , 24 , 25 , 26 ). This conceptual framework uses a system perspective and organizes variables into predisposing factors that shape attitudes toward health care utilization, need factors that encompass the individual's illness or impairment that necessitates service utilization, and enabling factors that refer to resources that promote or inhibit service use ( 23 ). As a framework for analysis, the social behavioral model does not dictate the exact variables and analytical methods that must be used. The appropriateness of variables to be included depends on the research question, the purpose of the study, and data availability ( 23 ). In addition to race and ethnicity, the data set used in this study contains other salient predisposing variables, including age and gender ( 26 , 27 , 28 ). Enabling factors are represented by school enrollment, city residency, and health insurance coverage ( 29 , 30 ). Need is assessed by several psychopathological measures, including severity of depression-related impairment, past-year delinquent behaviors, and substance abuse ( 31 , 32 , 33 ). The specific aims of this study were to investigate the extent to which racial or ethnic disparities exist between Caucasian and Hispanic youths in receiving adequate mental health care for past-year major depressive episodes and to examine the specific racial or ethnic factors that explain these disparities in receiving adequate mental health care. We hypothesized that among youths affected by past-year major depressive episodes, Caucasians would be more likely than Hispanics to receive adequate mental health care.
Methods
Data source and study sample
Data for this study were drawn from the 2005 National Survey on Drug Use and Health (NSDUH). The survey has been conducted since 1971 to provide estimates of substance use in the U.S. civilian population aged 12 and older. The NSDUH questionnaire was redesigned in the 1990s to place a greater emphasis on health status and health care, including access to mental health care ( 34 ). These data have been a useful tool for multidisciplinary studies ( 35 ). The 2005 NSDUH survey has a weighted screening response rate of about 90% and a weighted interview response rate of more than 80%. The interviews were conducted by using a combination of computer-assisted personal interviewing (CAPI), with responses entered by a field interviewer, and audio computer-assisted self-interviewing (ACASI), with responses entered privately by the participant. Details on the survey can be found elsewhere ( 36 ). The 2005 NSDUH contains 55,905 records covering equal proportions of persons aged 12–17, 18–25, and 26 years and older.
The 2005 NSDUH included a "youth depression" module to assess past-year major depressive episodes by using the diagnostic criteria set forth by the DSM-IV. Major depressive episode is defined as having at least five or more of nine DSM-IV clinical features nearly every day in the same two-week period, where at least one of the features was either a depressed mood or loss of interest or pleasure in daily activities ( 37 ). Questions were adapted from the depression section of the National Comorbidity Survey-Adolescent, which is based on a modified version of the World Health Organization Composite International Diagnostic Interview-Short Form (CIDI-SF) ( 38 ). In addition to good psychometric concordances between CIDI-SF and the full CIDI, clinical reappraisal analyses have shown agreement between CIDI diagnoses and independent clinician diagnoses ( 38 , 39 ). Moreover, the CIDI-SF is recommended to diagnose 12-month major depressive episodes in large-scale surveys ( 40 ). The sample used in this study included 1,485 Caucasians and Hispanics aged 12 to 17 years who were classified as affected by past-year major depressive episodes. The racial and ethnic distribution of the study sample was 1,169 (79%) Caucasians and 316 (21%) Hispanics.
Adequate mental health care
Respondents with past-year major depressive episodes were asked about their treatment experiences for depression during the past year, defined as "seeing or talking to a medical doctor or other health professional or taking prescription medication for major depressive episodes." All respondents were asked whether they received treatment or counseling during the past 12 months for emotional or behavioral problems that were not caused by alcohol or drugs at a mental health clinic or center; from a private therapist, psychologist, psychiatrist, social worker, or counselor; from an in-home therapist, psychiatrist, social worker, or counselor; or from a pediatrician or other family doctor. If respondents responded yes to any of the above questions, they were asked about the total number of visits to each of these providers. Other questions asked whether they received prescription medication for their depressive episodes.
Respondents who indicated that they received treatment were said to have received adequate mental health care if they received a prescription for an appropriate medication for depression, in combination with four or more visits to a psychiatrist, psychologist, general medical doctor, or other medical doctor, or if they were not psychotic, they received eight or more visits for depression-related problems with either a psychiatrist or another type of mental health specialist. This definition is based on evidence-based treatment guidelines that recommend a minimum of four visits for patients receiving medication during the acute and continuation phases for several types of mental disorders, including mood, anxiety, and psychotic disorders ( 17 , 41 ). In addition, clinical trials found that a minimum of eight sessions are needed with a mental health specialist in the absence of medication ( 19 , 42 , 43 ).
Coding of covariates
As discussed earlier, the covariate of primary interest in this study was race and ethnicity (Caucasian and Hispanic youths). We coded other covariates as follows: age (12–13, 14–15, and 16–17 years), gender (girls versus boys), school enrollment (enrolled versus not enrolled), and city residency (lived in a large Metropolitan Statistical Area or metropolitan area, in a small metropolitan area, or in a nonmetropolitan area).
We used the Sheehan Disability Scale to control for depression symptom severity ( 44 ). Analyses found high construct validity and internal consistency reliability for the Sheehan Disability Scale in assessing psychiatric impairment ( 45 ). The Sheehan Disability Scale is a measure of the impact of depression on a person's daily activities based on four domains in a person's life: chores at home, school or work, close relationships with family, and social life. Each domain uses an 11-point scale, in which 0 corresponds to no interference, 1 to 3 corresponds to mild interference, 4 to 5 corresponds to moderate interference, 7 to 9 corresponds to severe interference, and 10 corresponds to very severe interference. The data set included an overall impairment variable defined by the highest level of severity of role impairment reported across all four role domains. On the basis of the variable distribution, we construed a binary variable representing low interference (nil, mild, and moderate impairment) and high interference (severe and very severe impairment).
To control for delinquent behavior, we used an index based on six types of past-year delinquent acts ( 46 , 47 , 48 ): got into a serious fight at school or at work, took part in fight where group fights group, carried a handgun, attacked someone with intent to seriously hurt him or her, sold illicit drugs, and stole or tried to steal anything worth more than $50. Delinquent behaviors counts were grouped into three categories: none, one or two types, and three or more types ( 46 ). Measures for alcohol abuse (yes-no) and drug abuse (yes-no) were also included. Finally, we controlled for health insurance status (no insurance, private insurance, or public insurance—that is, Medicaid or State Children's Health Insurance Program [SCHIP]).
Statistical analysis
Univariate analyses were used to estimate the percentages of Caucasian and Hispanic youths in the sample who received adequate mental health care for past-year major depressive episodes. Nonparametric Kruskal-Wallis tests were used to assess the strength of the association between the covariates and receipt of adequate mental health care by race and ethnicity. Multivariable logistic regressions based on the full sample were used to assess the independent effects of race and ethnicity on receipt of adequate mental health care, adjusting for covariates. Multivariable logistic regressions were also estimated for each racial and ethnic group to examine correlates of receipt of adequate mental health care. All analyses were conducted with Stata software, release 9.0 ( 49 ). We used the "SVY" command, using weights provided in the data set to adjust for variations in within-household probabilities of selection and for differential nonresponse.
Results
Race and ethnicity and adequacy of treatment for depression
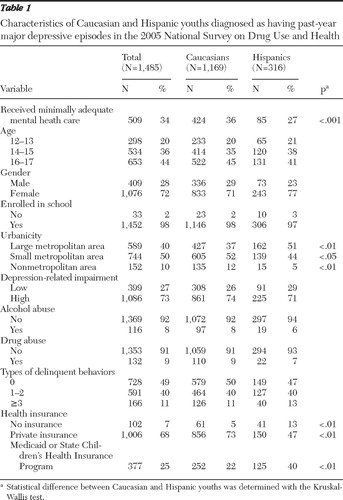
Table 1 shows the characteristics of the sample of Caucasian and Hispanic youths with past-year major depressive episodes. Thirty-four percent of the sample received adequate mental health care for major depressive episodes. Nonparametric Kruskal-Wallis test of significant differences indicated a higher proportion of Caucasians (36%) than Hispanics (27%) received adequate mental health care (p<.001). Moreover, we found that a majority of Hispanic youths lived in large metropolitan areas, while a majority of Caucasian youths lived in small or nonmetropolitan areas. The results also indicate that a significantly larger proportion of Caucasians had private insurance, whereas Hispanics were mostly uninsured or had Medicaid or SCHIP.
 |
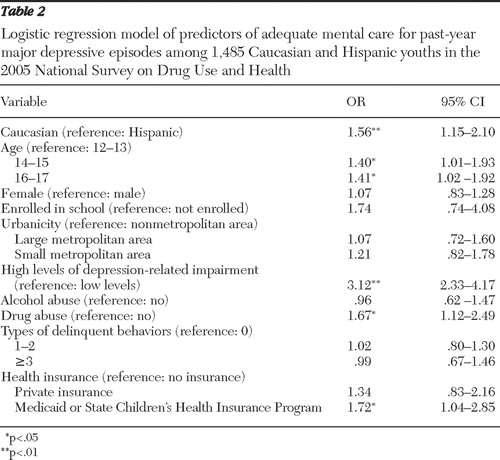
We analyzed the associations between race and ethnicity and receipt of adequate mental health care for past-year major depressive episodes. In the first logistic regression model, where race and ethnicity were entered alone, the results indicated that the odds of receiving adequate mental health care for Caucasians was 1.55 times that of Hispanics (odds ratio [OR]=1.55, 95% confidence interval, 1.17–2.03, p<.01). In the second logistic regression model that included all of the variables that were controlled for ( Table 2 ), the effect of race and ethnicity did not change (OR=1.56, p<.01). We also found that compared with respondents aged 12–13 years, those aged 14–15 years (OR=1.40, p=.04) and those aged 16–17 years (OR=1.41, p=.03) were more likely to receive adequate mental care. Youths with a high level of depression-related impairment had higher odds of receiving adequate mental health care, compared with those with a low level of depression-related impairment (OR=3.12, p<.01). Youths who abused drugs were more likely than those who did not to receive adequate mental health care for major depressive episodes (OR=1.67, p=.01). Having Medicaid or SCHIP increased the odds of receiving adequate mental health care (OR=1.72, p=.02), compared with having no insurance.
 |
Correlates of adequacy of treatment for depression
Caucasians.Table 3 shows the multivariable logistic models of adequate mental health care for Caucasian youths. Older Caucasians were more likely to receive adequate mental health care—that is, compared with Caucasians aged 12–13 years, the odds of receiving adequate mental care increased for youths aged 14–15 years (OR=1.69, p<.01) and for youths aged 16–17 years (OR=1.58, p=.01). The odds of receiving adequate mental health care increased for respondents who reported a high level of depression-related impairment, compared with those who reported a low level of depression-related impairment (OR=3.46, p<.01). Youths who abused drugs were more likely than those who did not to receive adequate mental care for major depressive episodes (OR=1.58, p=.04). Caucasian youths who had Medicaid or SCHIP were more likely than those with no insurance to receive adequate mental health care (OR=2.74, p<.004).
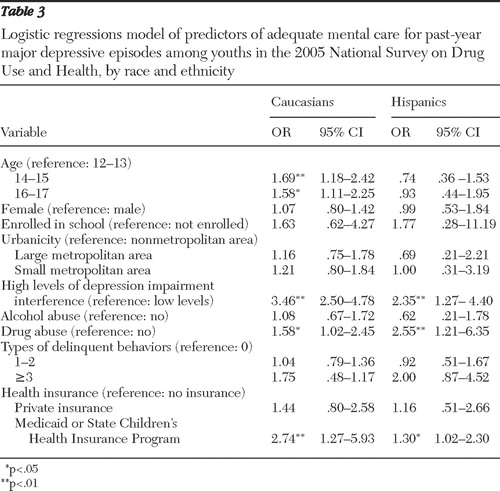 |
Hispanics.Table 3 also shows the multivariable logistic models of adequate mental health care for Hispanic youths. Much like our findings for Caucasian youths, we found that drug abuse increased the odds of receiving adequate mental health care for major depressive episodes among Hispanic youths (OR=2.55, p<.01). Also, the odds of receiving adequate mental health care increased for Hispanic youths who reported a high level of depression-related impairment, compared with those who reported a low level of depression-related impairment (OR=2.35, p<.01). Medicaid or SCHIP increased the odds of receiving adequate mental health care, compared with no insurance (OR=1.30, p<.05).
Discussion
This study examined disparities in receiving adequate mental health care among Caucasian and Hispanic youths affected by past-year major depressive episodes. Thirty-four percent of all youths in the sample received adequate mental health care. Our results are slightly lower than the 39% found for individuals aged 15 to 54 years who were shown to receive mental health care for serious mental illness in the National Comorbidity Survey ( 22 ). Separate analyses conducted for Caucasians and Hispanics in our study indicate that 36% of Caucasian youths received adequate mental care, compared with 27% of Hispanic youths. Logistic regressions indicate that Caucasian youths were 1.55 times as likely as Hispanic youths to receive adequate mental health care. Although previous research has not extensively examined racial or ethnic disparities in receiving adequate mental health care for major depressive episodes by using this working definition of a minimum of adequate mental care ( 20 , 21 ), our results are consistent with findings indicating that even when persons from racial or ethnic minority groups engage in mental services, they are more likely to make only a small number of visits to their providers ( 10 , 12 , 50 ).
Our results indicate that differences observed in adequate mental health care for depression among Caucasian and Hispanic youths persisted even after we controlled for other predisposing elements, enabling factors, and need for services in the Andersen model. Moreover, some of these factors that the analyses controlled for differ by race or ethnicity. The literature provides several plausible explanations for our findings within the Andersen framework. Previous research indicates that need factors such as presentation and interpretation of symptoms of mental disorders might differ according to race or ethnicity ( 51 ). Enabling culture and ethnic factors may prevent receipt of appropriate care among Hispanic youths even after they access mental health services ( 52 ). In addition, many persons from racial or ethnic minority groups mistrust the traditional care system and use more alternative treatment outside the health care system, such as pastoral and family counseling ( 53 , 54 ). All of these factors could reduce the likelihood that Hispanic youths would use an antidepressant prescription or return for a visit ( 52 ), which could also explain racial and ethnic disparities in adequate mental health care found in our study.
Having Medicaid or SCHIP significantly increased the odds of receiving adequate mental care for past-year major depressive episodes for both Hispanics and Caucasians. From a public policy standpoint, this finding indicates that public medical insurance is an important enabling tool for increasing receipt of adequate mental health care for youths. Financing for treating mental disorders has not increased commensurately with the rise in the numbers of youths affected by mental disorders ( 55 ). Medicaid or SCHIP benefits for treatment of mental disorders vary widely across states, and the emphasis is often on acute care services rather than on the relapsing condition of mental illness ( 56 ). As the financing burden continues to shift from the private sector to the public sector, new research is needed to examine the effects of publicly funded insurance on the effectiveness of service delivery systems for youths with mental disorders. Consistent with the findings of previous studies identifying impairment severity associated with mental disorder symptoms as a significant determinant of mental health care utilization ( 57 ), the results of our study showed that regardless of race or ethnicity, youths who reported severe depression-related impairment were more likely than those who did not to receive adequate mental health care. The results from the study presented here should be interpreted in light of its limitations. First, this study was based on cross-sectional data, and thus it is difficult to conclude that factors associated with receiving adequate mental health care are related causally. Second, the study used the "explicit mental health care" utilization concept, a relatively restricted definition of use that includes only services directly related to behavioral or emotional problems of youths ( 58 ). Third, we investigated receipt of adequate mental health care in formal outpatient settings. As noted earlier, persons from racial or ethnic minority groups frequently seek help for psychological problems from nonprofessional sectors, such as church and family, which could not be captured by the study presented here ( 53 , 54 ). Fourth, we examined data from Hispanics as a group, but there might be differences between Hispanics with origins from different countries (for example, Mexico versus Puerto Rico) and between Hispanics who are more acculturated and those who are less acculturated. Unfortunately, the NSDUH does not have data on acculturation. Finally, as with all self-report studies, there is also the possibility of recall bias. The NSDUH procedures are designed to maximize honesty and recall, and studies that examined the validity of data collected for the NSDUH found that the use of ACASI and CAPI methods produce more valid results than other self-report methods ( 59 ).
Conclusions
The study presented here investigated and found racial and ethnic disparities in receipt of adequate mental health care for past-year major depressive episodes among Caucasian and Hispanic youths. Previous research also found racial and ethnic disparities in mental health care for mental disorders ( 60 , 61 ). As more adolescents of diverse racial and ethnic backgrounds seek access to mental health treatment services, more study is needed about the degree to which treatment should be tailored to engage and retain racial and ethnic groups.
Acknowledgments and disclosures
This study was supported by two National Institute on Drug Abuse (NIDA) grants (AA-13608 and DA-020923). NIDA had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. The data reported were from the 2005 NSDUH public data files available at the Substance Abuse and Mental Health Data Archive and the Inter-university Consortium for Political and Social Research at University of Michigan ( webapp.icpsr.umich.edu ). The data collection and preparation were sponsored by the Office of Applied Studies, Substance Abuse and Mental Health Services Administration.
The authors report no competing interests.
1. Grob G: Mental health policy in twentieth-century America; in Mental health, United States, 2000. Edited by Manderscheid RW, Henderson MJ. Rockville, Md, Substance Abuse and Mental Health Services Administration, 2001Google Scholar
2. Levin BL, Petrila J, Henessy KD: Mental Health Services: A Public Health Perspective, 2nd ed. New York, Oxford University Press, 2004Google Scholar
3. Ringel JS, Sturm R: Financial burden and out-of-pocket expenditures for mental health across different socioeconomic groups: results from healthcare for communities. Journal of Mental Health Policy and Economics 4:141–150, 2001Google Scholar
4. Ringel JS, Sturm R: National estimates of mental health utilization and expenditures for children in 1998. Journal of Behavioral Health Services and Research 28:319–333, 2001Google Scholar
5. Leaf PJ, Alegria M, Cohen P, et al: Mental health service use in the community and schools: results from the four-community MECA study. Journal of the American Academy of Child and Adolescent Psychiatry 35:889–897, 1996Google Scholar
6. Cuffel BJ, Held M, Goldman W: Predictive models and the effectiveness of strategies for improving outpatient follow-up under managed care. Psychiatric Services 53:1438–1443, 2002.Google Scholar
7. Snowden LR: Racial differences in informal help seeking for mental health problems. Journal of Community Psychology 26:429–438, 1998Google Scholar
8. Lopez SR: A research agenda to improve the accessibility and quality of mental health care for Latinos. Psychiatric Services 53:1569–1573, 2002Google Scholar
9. Freedenthal S: Racial disparities in mental health service use by adolescents who thought about or attempted suicide. Suicide and Life-Threatening Behavior 37:22–34, 2007Google Scholar
10. Lavigne JV, Arend R, Rosenbaum D, et al: Mental health service use among young children receiving pediatric primary care. Journal of the American Academy of Child and Adolescent Psychiatry 37:1175–1183, 1998Google Scholar
11. Padgett DK, Patrick C, Burns BJ: Ethnicity and the use of outpatient mental health services in a national insured population. American Journal of Public Health 84:222–226, 1994Google Scholar
12. Harpaz-Rotem I, Leslie D, Rosenheck RA: Treatment retention among children entering a new episode of mental health care. Psychiatric Services 55:1022–1028, 2004Google Scholar
13. Rosenheck R, Massari L, Frisman L: Who should receive high-cost mental health treatment and for how long? Schizophrenia Bulletin 19:843–852, 1993Google Scholar
14. Wells RB, Sherbourne C, Schoenbaum M, et al: Impact of disseminating quality improvement programs for depression in managed primary care. JAMA 283:212–220, 2000Google Scholar
15. Melfi CA, Chawla AJ, Croghan TW, et al: The effect of adherence to antidepressant treatment guidelines on relapse and recurrence of depression. Archives of General Psychiatry 55:1128–1132, 1998Google Scholar
16. Katon W, Von Korff M, Lin E. et al: Collaborative management to achieve treatment guidelines: impact on depression in primary care. JAMA 273:1026–1031, 1995Google Scholar
17. Depression in Primary Care, Vol 2: Treatment of Major Depression. Rockville, Md, Agency for Healthcare Research and Quality, 1993Google Scholar
18. Practice Guideline for Major Depressive Disorder in Adults. Washington, DC, American Psychiatric Publishing, 1993Google Scholar
19. Lehman AF, Steinwachs DM: Translating research into practice: the Schizophrenia Patient Outcomes Research Team (PORT) treatment recommendations. Schizophrenia Bulletin 24:1–10, 1998Google Scholar
20. Borges G, Elena Medina-Mora M, Wang PS, et al: Treatment and adequacy of treatment of mental disorders among respondents to the Mexico National Comorbidity Survey. American Journal of Psychiatry 163:1371–1378, 2006Google Scholar
21. Wang PS, Demler O, Kessler RC: Adequacy of treatment for serious mental illness in the United States. American Journal of Public Health 92:92–98, 2002Google Scholar
22. Harrington R, Rutter M, Fombonne E: Developmental pathways in depression: multiple meanings, antecedents, and endpoints. Developmental Psychopathology 8:601–616, 1996Google Scholar
23. Andersen RM: Revisiting the behavioral model and access to medical care: does it matter? Journal of Health and Social Behavior 6:1–10, 1995Google Scholar
24. Elhai JD, Ford JD: Correlates of mental health service use intensity in the National Comorbidity Survey and National Comorbidity Survey Replication. Psychiatric Services 58:1108–1115, 2007Google Scholar
25. Wu P, Christina WH, Patricia C, et al: Factors associated with use of mental health services for depression by children and adolescents. Psychiatric Services 52:189–195, 2001Google Scholar
26. Keyes KM, Hatzenbuehler ML, Alberti P, et al: Service utilization differences for axis I psychiatric and substance use disorders between Caucasian and black adults. Psychiatric Services 59:893–901, 2008Google Scholar
27. Wang PS, Lane M, Olfson M, et al: Twelve-months use of mental health services in the United States: results from the National Comorbidity Survey Replication (NCS-R). Archives of General Psychiatry 62:629–640, 2005Google Scholar
28. Rhodes AE, Goering PN, To T, et al: Gender and outpatient mental health service use. Social Science and Medicine 54:1–10, 2002Google Scholar
29. Sourander A, Multimaki P, Santalahti P, et al: Mental health service use among 18-year-old adolescent boys: a prospective 10-year follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry 43:1250–1258, 2004Google Scholar
30. Zwaanswijk M, van der Ende J, Verhaak PF, et al: Factors associated with adolescent mental health service need and utilization. Journal of the American Academy of Child and Adolescent Psychiatry 42:692–700, 2003Google Scholar
31. Alegria M, Kessler RC, Bijl R, et al: Comparing data on mental health service use between countries; in Unmet Needs in Psychiatry: Problems, Resources, Responses. Edited by Andrews G, Henderson S. Cambridge, England, Cambridge University Press, 2000Google Scholar
32. Briggs-Gowan MJ, Horwitz SM, Schwab-Stone ME, et al: Mental health in pediatric settings: distribution of disorders and factors related to service use. Journal of the American Academy of Child and Adolescent Psychiatry 39:841–849, 2000Google Scholar
33. Horwitz SM, Gary LC, Briggs-Gowan MJ, et al: Do needs drive services use in young children? Pediatrics 112:1373–1378, 2003Google Scholar
34. Preliminary Estimates From the 1994 National Household Survey on Drug Abuse. Rockville, Md, Substance Abuse and Mental Health Services Administration, 1995Google Scholar
35. Kessler RC, Barker PR, Colpe LJ, et al: Screening for serious mental illness in the general population. Archives of General Psychiatry 60:184–189, 2003Google Scholar
36. Results From the 2005 National Household Survey on Drug Abuse: Technical Appendices and Selected Data Tables: Public Release. Rockville, Md, Substance Abuse and Mental Health Services Administration, 2006Google Scholar
37. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC, American Psychiatric Publishing, 1994Google Scholar
38. Kessler RC, Andrews G, Mroczek D, et al: The World Health Organization Composite International Diagnostic Interview Short Form (CIDI-SF). International Journal of Methods in Psychiatric Research 7:171–185, 1998Google Scholar
39. Wittchen HU: Reliability and validity studies of the WHO-Composite International Diagnostic Interview (CIDI): a critical review. Journal of Psychiatric Research 28:57–84, 1994Google Scholar
40. Aalto-Setala T, Marttunen MJ, Tuulio-Henriksson A: Depressive symptoms in adolescence as predictors of early adulthood depressive disorders and maladjustment. American Journal of Psychiatry 159:1235–1237, 2003Google Scholar
41. Wang PS, Berglund PA, Kessler RC: Recent care of common mental disorders in the US: prevalence and conformance with evidence-based recommendations. Journal of General Internal Medicine 15:284–292, 2000Google Scholar
42. Practice Guideline for the Treatment of Patients With Panic Disorder. Washington, DC, American Psychiatric Publishing, 1998Google Scholar
43. Practice Guideline for the Treatment of Patients With Schizophrenia. Washington, DC, American Psychiatric Publishing, 1997Google Scholar
44. Sheehan DV, Sheehan KE: The classification of anxiety and hysterical states. Journal of Clinical Psychopharmacology 2:235–243, 1982Google Scholar
45. Leon AC, Olfson M, Portera L, et al: Assessing psychiatric impairment in primary care with the Sheehan Disability Scale. International Journal of Psychiatry Medicine 27:93–105, 1997Google Scholar
46. Wu LT, Howard MO: Is inhalant use a risk factor for heroin and injection drug use among adolescents in the United States? Addictive Behaviors 32:265–281, 2007Google Scholar
47. Smith D, Davidson L: Interfacing indicators and constructs in criminological research: a note on the comparability of self-report violence data for race and sex groups. Criminology 24:473–488, 1986Google Scholar
48. Hinderlang M, Hirschi T, Weis J: Measuring Delinquency. Sage, Beverly Hills, Calif, 1981Google Scholar
49. Stata Reference Manual: Release 9. Texas, Stata Corp, 2005Google Scholar
50. Alexandre PK: Mental health care for youth: predictors of use are not always the same as predictors of volume. Social Science Journal 45:619–632, 2008.Google Scholar
51. Baker FM, Bell CC: Issues in the psychiatric treatment of African Americans. Psychiatric Services 50:362–368, 1999Google Scholar
52. Merritt-Davis OB, Keshavan MS: Pathways to care for African-Americans with early psychosis. Psychiatric Services 57:1043–1044, 2006Google Scholar
53. McMiller WP, Weisz JR: Help-seeking preceding mental health clinic intake among African-American, Latino and Caucasian youth. Journal of the American Academy of Child and Adolescent Psychiatry 35:1086–1094, 1996Google Scholar
54. Chalfant PH, Peter HL, Alden R: The clergy as a resource for those encountering psychological distress. Review of Religious Research 31:305–313, 1990Google Scholar
55. American Academy of Pediatrics, Committee on Child Health Financing and Committee on Substance Abuse: Improving substance abuse prevention, assessment, and treatment financing for children and adolescents. Pediatrics 108:1025–1029, 2001Google Scholar
56. Johnson P: Substance Abuse Treatment Coverage in State Medicaid Programs. Washington, DC, National Conference of State Legislatures, 1999Google Scholar
57. Booth BM, Cook AL, Blow FC: Utilization of outpatient mental health services after inpatient alcoholism treatment. Journal of Mental Health Administration 19:21–30, 2002Google Scholar
58. Olfson M, Pincus HA: Outpatient psychotherapy in the United States. I: volume, costs, and user characteristics. American Journal of Psychiatry 151:1281–1288, 1994Google Scholar
59. Harrison L: The validity of self-reported drug use in survey research: an overview and critique of research methods. NIDA Research Monograph 167:17–36, 1997Google Scholar
60. Dakof GA: Understanding gender differences in adolescent drug abuse: issues of comorbidity and family functioning. Journal of Psychoactive Drugs 32:25–32, 2000Google Scholar
61. Robbins MS, Kumar S, Walker-Barnes C, et al: Ethnic differences in comorbidity among substance-abusing adolescents referred to outpatient therapy. Journal of the American Academy of Child and Adolescent Psychiatry 41:394–401, 2002Google Scholar

