
Datapoints: The Ups and Downs of Dosing Second-Generation Antipsychotics
Dosing of second-generation antipsychotics involves achieving efficacy while minimizing adverse effects. Increasing the daily dosage may reduce psychopathology but may cause risks. The use of high dosing for olanzapine and quetiapine has been previously noted ( 1 ). We now have additional information on the dosing patterns of the two newest second-generation antipsychotics, ziprasidone and aripiprazole.
We report the percentage of patients hospitalized within the inpatient facilities operated by the New York State Office of Mental Health who received high dosages of ziprasidone and aripiprazole from January 1, 2001, to June 30, 2006. Approximately 5,000 patients received antipsychotics of any kind within any calendar quarter. A complete description of the database used and the methodology employed has been published elsewhere ( 1 ).
Figure 1 displays the percentage of patients in each quarter who received a daily dosage of ziprasidone or aripiprazole in excess of 160 mg/day and 30 mg/day, respectively. For comparison the figure also shows the percentage of patients receiving high dosages of olanzapine or quetiapine.
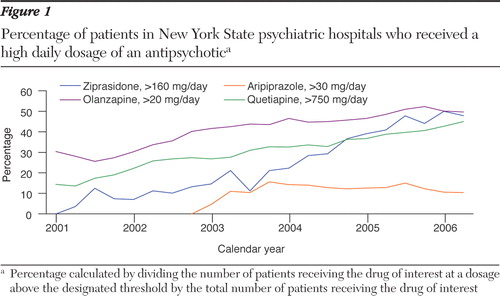
The observation that ziprasidone was being used at high dosages may be due to a possible dose-response relationship that results in greater efficacy with higher dosages than the dosages tested during the registration process. We can also hypothesize that higher dosing of ziprasidone occurred because of lower bioavailability when not taken with food, possibly leading clinicians to use higher dosages in order to compensate for medication administration occurring between meals ( 2 ).
In contrast to ziprasidone, the use of high doses of aripiprazole is uncommon. A possible explanation may lie in its mechanism of action as a partial agonist at the D2 receptor ( 3 ), with this dopamine "stabilizing" effect preventing further D2 blockade with higher dosages.
The nature of the observational data presented here does not allow us to directly test whether higher dosages of antipsychotics are any more efficacious than lower ones. There remains a need for well-designed studies that examine the response to fixed dosages of second-generation antipsychotics.
Acknowledgments and disclosures
Partial support for the maintenance of the integrated research database is currently being provided by unrestricted grants from AstraZeneca and Eli Lilly and Company.
Dr. Citrome reports receiving honoraria or research support from Abbott Laboratories, AstraZeneca Pharmaceuticals. Barr Laboratories, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, Janssen Pharmaceuticals, Jazz Pharmaceuticals, and Pfizer. Dr. Jaffe reports receiving research support from Eli Lilly and Company. Dr. Levine reports no competing interests.
1. Citrome L, Jaffe A, Levine J: Dosing of second-generation antipsychotic medication in a state hospital system. Journal of Clinical Psychopharmacology 25:388-391, 2005Google Scholar
2. Hamelin BA, Allard S, Laplante L, et al: The effects of timing of a standard meal on the pharmacokinetics and pharmacodynamics of the novel atypical antipsychotic agent ziprasidone. Pharmacotherapy 18:9-15, 1998Google Scholar
3. Burris KD, Molski TF, Xu C, et al: Aripiprazole, a novel antipsychotic, is a high-affinity partial agonist at human dopamine D2 receptors. Journal of Pharmacology and Experimental Therapeutics 302:381-389, 2002Google Scholar

