
Research on Day Treatment Programs for Preschoolers With Disruptive Behavior Disorders
Day treatment programs have been a mainstay of psychiatric intervention among preschoolers since the mid-20th century. Also referred to as partial hospitalization, these programs provide intensive treatment in a group setting for several hours weekly, usually with educational and recreational components. In the Canadian province of Quebec, more than 200 preschoolers are treated in day treatment programs at any one time, and most of these children are referred for treatment of behavioral problems ( 1 ). However, this mode of intervention has seldom appeared in the literature.
The effectiveness of day treatment for preadolescent children with disruptive behavior disorders (that is, oppositional defiant disorder or conduct disorder) has been reported ( 2 ), but few studies have been published specific to the preschool age group. Developmental and contextual differences (for example, language skills and academic demands) limit the applicability of evidence on programs for older children to programs for preschoolers. Also, day treatment studies have described preschoolers as having behavior problems but have not used DSM-IV criteria for diagnosing disruptive behavior disorder, again limiting comparisons with studies of preadolescent children. One of the few available studies of preschool day treatment did not find positive treatment effects ( 3 ). More evidence is clearly needed in this area.
General features of day treatment programs
The "containing" function of a therapeutic milieu has been widely recognized as a mediator of change in psychiatry. The milieu allows for a prolonged assessment of a child's difficulties and of complex family systems. A day treatment center may be the only place where disruptive children and their families find acceptance, because these children are often rejected by peers, schools, and other caregivers because of their behavior ( 4 ). McDermott and colleagues ( 5 ) ascertained that children whom psychiatrists assign to day treatment have more psychopathology, clinician-rated impairment, and parental mental health and substance abuse issues than children assigned to other treatments. Many children are referred to day treatment centers because their needs could not be met with community or outpatient resources ( 6 ).
Most day treatment programs are multimodal, addressing multiple areas of difficulty for a child or within the family with a combination of treatment modalities. Smolla and Lebel ( 1 ) suggested that the specific mandate of day treatment is to provide integrated care from multiple specialists targeting not only behavioral problems but also emotional issues, developmental delays, and contributory medical problems. A high correlation between behavioral problems and developmental and language delays has been found ( 7 , 8 , 9 , 10 ), and two-thirds of children in day treatment may have such delays ( 6 , 11 ). It is possible that day treatment programs serve preschoolers with both behavior problems and developmental delays in a uniquely efficient manner, but little research supports this notion. Not all day treatment programs are able to include speech therapists, occupational therapists, and physiotherapists on their treatment teams ( 1 ).
Children in day treatment are a captive audience for intensive intervention ( 12 ), particularly in programs requiring attendance on multiple days per week. The actual interventions offered differ from center to center and from country to country. A 1986 American survey found that most day treatment centers for children use a behavioral approach (33 percent) or describe themselves as eclectic (34 percent), whereas a 1988 survey in France found that most day centers operate with a psychoanalytic framework ( 13 , 14 ). A survey of day treatment centers for children in Quebec found that 42 percent claimed a psychodynamic orientation ( 1 ). Family therapy is an integral part of most programs and is mandatory in some.
Day treatment programs and evidence-based practice
As the number of child psychosocial interventions developed in research settings (laboratory-based interventions) grows, attention has increased on integrating these interventions into service-oriented clinical settings, such as day treatment programs ( 15 ). However, it is unclear for most of these laboratory-based interventions whether they are superior to interventions currently employed in clinical settings (clinic-based interventions), because outcome data are rarely available for the latter. Also, it is problematic to compare laboratory-based interventions that have a single treatment focus to clinic-based interventions that often target multiple treatment goals.
Weisz and colleagues ( 12 ) commented on the gap between laboratory-based and clinic-based research in child psychotherapy, finding dismal outcomes from nine clinical studies identified in an extensive literature search, which contrasted with large effect sizes from more than 100 laboratory studies. They found that the difference in outcomes was partly influenced by the relative treatability of children in the laboratory studies. The disparity in treatability may be most apparent when children recruited for laboratory-based studies are compared with children in clinic-based day treatment studies. Children in the latter group may be assigned to day treatment because of the severity of their impairment and may not be eligible for less intensive interventions, such as those offered in research settings. Differences in outcome between laboratory- and clinic-based studies are also influenced by superior conditions in research settings and whether behavioral methods were used in research therapies. Weisz and colleagues proposed that treatment effects by practitioners in clinical settings need to be examined and laboratory-tested interventions need to be applied in clinics.
Integrating laboratory-based interventions into service-oriented clinical settings is by no means a simple task. Kazdin ( 15 ) identified several barriers to integration, including issues surrounding the quality of available evidence, disparate views among stakeholders in treatment, and lack of resources for training therapists. Ollendick and King ( 16 ) discussed controversy around manualized treatments, including acceptability to clinicians and flexibility to accommodate specific clinical situations.
This review attempts to aid in the integration process by delineating practical ways of using research findings to enhance clinical work. First, the available evidence for effectiveness of clinical preschool day treatment programs was reviewed to demarcate a starting point for future research in this area. Then laboratory-based interventions offering accessible solutions to common clinical issues in preschool day treatment were selected for discussion. This review focused on psychosocial interventions for disruptive behaviors. The growing evidence base in this area appears to have the most to offer to preschoolers in day treatment, for whom behavior problems are most often the presenting complaint.
Methods
Reports on the effectiveness of clinic-based multimodal day treatment programs or on the efficacy of laboratory-based child psychosocial interventions were found by performing a PsycINFO computerized search covering the past 30 years (1974 to 2004). The keywords "day treatment," "behavior problems," "disruptive behavior disorder" and "oppositional defiant disorder" were used, and the search was limited to the preschool age group (ages two to five years). The reference lists of articles found were then manually searched. A MEDLINE search was also performed but yielded a lower proportion of articles pertinent to the objective of this review.
The initial intent was to include only randomized controlled trials for review. However, only one randomized controlled trial of a clinic-based multimodal day treatment program was found. The study selection criteria were therefore modified for day treatment programs, so that articles were selected if they had a prospective design and presented quantitative outcome data. For laboratory-based interventions, only randomized controlled trials were selected.
Reports on specialized day treatment programs for children with autism or intellectual delay were excluded, because such programs are beyond the scope of this review. Reports on specialized interventions for children with attention-deficit hyperactivity disorder were also excluded, because this diagnosis was not described in the studies of preschool day treatment programs that were found.
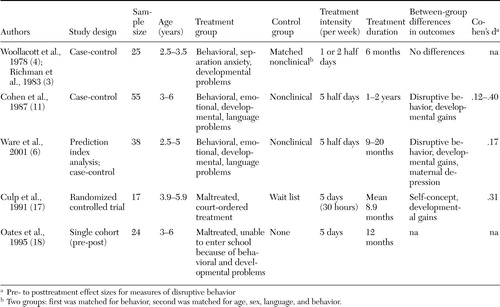
Characteristics of selected studies are summarized in Tables 1 , 2 , 3 , 4 , 5 . Effect sizes (Cohen's d) have been calculated where means and standard deviations on measures of disruptive behaviors were provided. Differences in the nature of the study sample and duration of follow-up are some of the factors to be considered when comparing study effect sizes.
 |
 |
 |
 |
 |
Results
Reports on the effectiveness of selected clinic-based multimodal day treatment programs are summarized, followed by an overview of reports on the efficacy of laboratory-based preventive, child-oriented, parent training and classroom-based interventions.
Effectiveness of clinic-based multimodal day treatment programs
Only five studies of preschool day treatment programs were found that reported quantitative outcomes, for a combined total of 159 children. Study characteristics are summarized in Table 1 .
In one of the earliest studies of day treatment, Woollacott and colleagues ( 4 ) described children referred to a therapeutic nursery that emphasized parent-oriented interventions. Mothers interacted with their children in the nursery, where the focus was on parental attunement and mother-child communication. A mothers' support group and social work liaison were also offered. The treatment group made no more gains than matched children in the nonclinical control group at one- and five-year follow-up ( 3 , 4 ).
Cohen and colleagues ( 11 ) reported on a prescriptive multifocused treatment program for preschoolers. A variety of interventions were employed, according to the treatment goals of each child. These could include setting limits, helping the child to verbalize feelings, and implementing speech therapy, among other things. Families were expected to observe and work with their children in the playroom and were seen regularly by a social worker. Behavior changes were found only among children who remained in the program more than one year. Children who had both behavioral problems and developmental delays made more gains than children without developmental delays. Family motivation was correlated with goal attainment. Little change was found for the nonclinical control group.
Ware and colleagues ( 6 ) reported on a psychodynamically oriented program involving special education, individual and group play therapy, and weekly family therapy. On measures of daily living skills—socialization and visual-motor integration with established age-based norms—significant gains in developmental level were found, compared with gains that could be predicted on the basis of change in the child's age. Other uncontrolled pre- to posttreatment gains in behavior and parental functioning were found. On follow-up in first and third grade, graduates of the program needed less special education than children with similar problems identified in kindergarten (an unmatched comparison group).
Two of the programs described in the literature search were developed to address behavioral and emotional problems among children who had been physically or sexually abused. In one program, maltreated preschoolers received a specialized curriculum emphasizing feelings and relationships ( 17 ). The preschoolers also received individual play therapy, speech therapy, and physical therapy. Their parents received intensive services, including family therapy, education, and a 24-hour crisis line. A randomized controlled study found increased peer acceptance and developmental gains for children who received this program. In this study use of a wait list control group was justified, because participation in the program was mandated by judicial order, but space in the program was limited.
The second program provided maltreated preschoolers with a curriculum emphasizing limit setting and consistency, along with individual psychotherapy ( 18 ). Parents were supported through regular home visits. The success of the program was determined by school entrance after a year of treatment. Developmental gains were also reported, but no comparison group was available.
These day treatment studies offered a range of interventions, with children in each study receiving different interventions. Few specifications were given for diagnoses of children in these studies. Different outcome measures and methods of comparison were used. Therefore, it is difficult to derive meaningful conclusions about the effectiveness of day treatment programs by examining these reports. It is not possible to know whether the one negative study did not find between-group differences because the intervention was ineffective or because the control group was poorly matched. Only one study employed a truly comparable (randomized) control group.
On a very general level, it is possible to conclude that modest evidence shows that multimodal day treatment programs can be effective. Treatment tends to result in developmental gains. One commonality of the programs described was that they all expected families to be involved. Only one study made any suggestion about the effect of duration of treatment or type of child problem on effectiveness ( 11 ). No information on the effect of treatment intensity could be found, and no comparisons were made with conventional outpatient treatment. It appears that the research base for this costly and intensive model of service delivery is lacking.
Efficacy of laboratory-based interventions
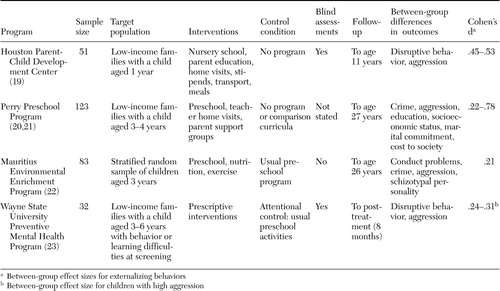
Efficacy of multimodal prevention programs. Four randomized controlled trials of multimodal prevention programs for preschoolers were found. These programs recruited low-income families, based on findings that socioeconomic status is associated with antisocial characteristics. The studies are summarized in Table 2 .
The Houston Parent-Child Development Center offered a two-year program involving home visitation, parent training, preschool education, and family workshops ( 19 ). A broad range of other resources were available, including stipends, meals, and transportation. Positive child behavioral and family socioeconomic outcomes were found on follow-up up to eight years later.
The Perry Preschool Program also combined high-quality child education with home visitation. Parent support groups were offered as well. Decreased delinquency and improved academic and employment outcomes were found up to age 27 for individuals who had attended the Perry Preschool Program. Costs from crime were reduced by about $70,000 per child ( 20 , 21 ).
These primary prevention strategies were exported to Mauritius in the Environmental Enrichment Program, where preschoolers were randomly selected to receive a two-year program of nutrition, education, and exercise ( 22 ). Many of these children were malnourished upon entry to the program. Lower rates of antisocial behavior and schizotypy were found up to 26 years of age for individuals who went through the preschool program.
Wayne State University's Preventive Mental Health Program employed a prescriptive approach, similar to the prescriptive multifocused treatment offered in the clinic-based day treatment study of Cohen and colleagues ( 11 ). In this prevention program, preschoolers found on screening to have learning and behavioral difficulties were randomly assigned to receive either customized behavioral interventions or "placebo attention" in addition to their regular preschool program ( 23 ). Between-group differences were found in behavior and academic functioning at the end of the eight-month program.
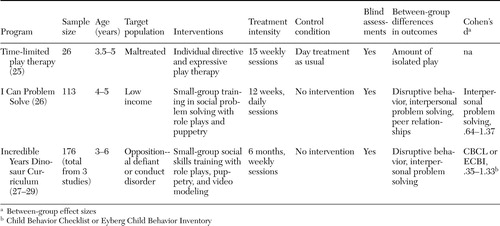
Efficacy of child-oriented interventions. Several training programs focusing on social, anger-management, and problem-solving skills have been developed for children, but only two had been tested in randomized controlled trials with preschool-aged children: I Can Problem Solve and the Incredible Years Dinosaur Curriculum. These programs target aberrant social cognition, which has been implicated in the pathogenesis of conduct disorder ( 24 ). Only one randomized controlled study of child psychodynamic therapy was found ( 25 ). This study found no significant effects on behavioral measures when individual play therapy was added to a day treatment program. These three studies are summarized in Table 3 .
I Can Problem Solve is a three-month small-group program teaching preschoolers interpersonal problem-solving skills and emotional literacy, using puppetry and role-play games to promote learning ( 26 ). Improved classroom behavior, peer relationships, and interpersonal problem solving were found for preschoolers who received the program as a preventive intervention. Positive outcomes were maintained at follow-up in grade five to six.
The Dinosaur Curriculum adapts the principles guiding I Can Problem Solve to treat children referred with conduct problems. Children meet in small groups for two hours each week for 22 weeks. The multimedia sessions employing videos and life-size puppets emphasize emotional literacy, empathy, friendship skills, anger management, interpersonal problem solving, and school success. Three randomized controlled trials showed decreases in peer aggression and noncompliant behavior and increased prosocial and problem-solving skills among children who received the curriculum ( 27 , 28 , 29 ).
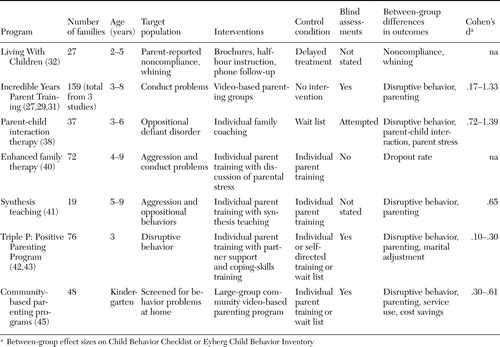
Efficacy of parent training interventions. Parent training has been robustly supported in the literature on treatments for disruptive behavior disorders. Several parent training programs have been tested in randomized controlled trials that include preschool-aged children. These trials are summarized in Table 4 . They are organized here to highlight aspects that may inform clinical family-oriented services.
Brestan and Eyberg ( 30 ) deemed only two treatment programs to be "well established" in their review of 82 studies of psychosocial treatments for children. One was the Living With Children manual, and the other was the Incredible Years videotape modeling parent training program ( 27 , 29 , 31 , 32 ). Both programs teach parents to monitor and reward positive behaviors and to ignore and give consequences for deviant behaviors. Timeouts are an important part of both programs; this behavioral technique has been found to be essential in a randomized controlled trial ( 33 ). Parental self-control and self-talk techniques are emphasized in the Incredible Years program. Living With Children is designed for the training of individual families but has been adapted for group training ( 34 ), whereas the Incredible Years program is designed for groups but can be self-administered ( 35 ).
The content of most parent training programs is similar, rooted in social learning principles, but several studies have suggested that program format and delivery may have an effect on training effectiveness. For example, families that were randomly assigned to receive the Incredible Years videotape modeling parent training in a self-administered format had more difficulties at the three-year follow-up than families who received the training with therapist-led group discussion after each videotaped vignette ( 31 , 35 ). Families randomly assigned to receive only the therapist-led discussion did not fare as well as the group that received both the videotape modeling parent training and therapist-led discussion. Of note, studies of the Incredible Years parenting program tend to have dropout rates of less than 10 percent, whereas dropout among families referred to parent management programs is usually in the range of 50 to 75 percent ( 36 , 37 ).
Another program enhanced by technology is parent-child interaction therapy, in which therapists coach parents through a "bug-in-the-ear" earphone from behind a one-way mirror. Parent-child interaction therapy has been extensively tested, with findings that clinically significant behavior changes in treated preschoolers are maintained up to six years later ( 38 , 39 ). However, no studies comparing parent-child interaction therapy with other therapies were found.
Enhancing the content of programs for parents may also influence their engagement in therapy. Lower dropout rates were found for families that were randomly assigned to a standard (social-learning-based) family therapy enhanced by therapists' solicitation of parents' feelings and concerns, compared with families that received the family therapy alone ( 40 ).
Synthesis teaching, in which parents are trained to discriminate child care stresses from stress from other sources and to examine similarities between the ways that they respond to their child and to other people, was more efficacious than unenhanced parent training in improving parenting and child behavior ( 41 ).
Studies of the Triple P: Positive Parenting Program found that a marital communication skills program (partner support training) added to a parent training program enhanced treatment gains for families with marital discord ( 42 ). However, differences in outcome were limited when all families were included, and no difference was found in dropout rates ( 43 ). Webster-Stratton ( 44 ) also found that, although skills training in marital communication enhanced parental functioning, it did not improve child behavior outcomes. The Triple P research group concluded that there may be limited benefit in offering targeted interventions for parental distress to all referred families.
Practical factors have also been implicated in parent engagement in therapy. Location may be an important factor for some families: those whose first language was not English and who had children with more severe problems were more likely to participate in a community-based parenting program if it was held in a school rather than in a medical center ( 45 ). Financial compensation, flexible scheduling, and reminder letters have also been used to increase parental compliance ( 38 ).
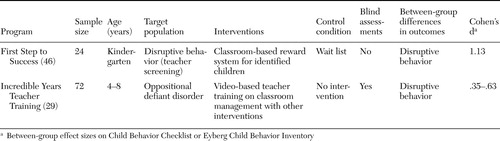
Efficacy of classroom-based interventions. As shown in Table 5 , two classroom-based programs were found that had been tested in randomized controlled trials that included preschool-aged children. The Contingencies for Learning Academic and Social Skills program (CLASS) has been adapted for kindergarten-age children ( 46 ). This intervention involves awarding points to a disruptive child for on-task behavior. Essentially, CLASS manualizes the social-learning principles of monitoring, contingent attention, and reinforcement for use in a classroom setting. In the First Step to Success program, CLASS increased on-task behavior among children identified with behavior problems.
The Incredible Years Teacher Training program also facilitates teachers' integration of social-learning principles into classrooms. Teachers attend workshops that last four to six days and offer a video-based curriculum on classroom management skills and relationship building with students and their parents. Improved classroom behavior was found for children whose teachers received training ( 29 ).
Discussion
Little research was found to support the use of multimodal preschool day treatment, despite its prevalence in clinical practice. Many questions remain as to the optimal design of these programs. In the meantime, it seems reasonable to optimize effectiveness by finding ways to incorporate elements of empirically supported interventions into day treatment programs. Some lessons from laboratory-based interventions are discussed below, with suggestions for clinical practice and future study.
Lessons from multimodal prevention programs
With multimodal prevention programs, as with day treatment programs, it is difficult to determine which interventions contributed to the outcomes. However, the prevention programs described have some important commonalities. First, all programs offered preschool education. The day treatment programs, on the other hand, emphasized education to different degrees, with apparently minimal content in some programs. Children who have difficulty learning because of behavioral or developmental delays likely benefit from assertive efforts to provide early preparation for grade school. Day treatment programs could be a place where children who are unable to attend community preschools can receive high-quality education.
Second, two of the prevention programs included home visitation. Economically stressed families may be more amenable to interventions that are provided in their own milieu, particularly if lack of transportation impedes their access to resources. In addition, home visitation may give clinicians a better sense of a family's needs. Only one of the day treatment programs reviewed offered regular home visits as part of their program ( 18 ). Home visitation requires clinician time and flexibility, which may not be readily available in already overextended programs. Also, many day treatment programs may be unable to provide transportation. However, this intervention may be necessary for certain children to participate in treatment ( 1 ).
Two of the prevention programs also met very basic needs of children and families: nutrition, health care, and economic support. It may be that only by addressing families' practical needs can we reach the large proportion of families who do not benefit from traditional treatment approaches ( 31 ). Addressing these needs not only lays the foundation for healthy child development but also fosters a therapeutic relationship with the child's family. A lunch program may help some families. Physical activity should be part of day treatment programming. Day treatment teams would do well to include a social worker and maintain close liaisons with pediatricians.
Finally, it is clear from studies on prevention programs that supporting families in children's early years may have measurable effects on outcomes even in adulthood. Although no clinic-based day treatment studies have followed children into adulthood, it is reasonable to speculate that intervening to change a child's course early on may have an enduring effect on his or her development, achievements, and relationships. If so, then the quality of care that we provide to disruptive preschoolers should be optimized.
Lessons from child-oriented interventions
Elements of social-skills and problem-solving training may be implicitly present in existing day treatment programs. For example, two day treatment programs taught children to identify and verbalize their feelings. However, the explicit introduction of skills, using specific methods to promote skill acquisition and generalization, may be less common in day treatment settings.
Manualized programs, such as I Can Problem Solve and the Incredible Years Dinosaur Curriculum, offer a coherent method of delivering social skills training to preschoolers, using techniques that have been designed to engage children. Day treatment programs may find prepared materials for role-play games, puppetry, and videotapes showing modeling behavior helpful in maintaining children's attention. Manualized curricula could also be offered to preschoolers as distinct modules in day treatment programs.
Many child clinicians find psychodynamic therapies to be useful, and many day treatment programs report a psychodynamic orientation ( 1 , 47 ) However, the only study of play therapy found was negative. It may be premature to conclude from this one study that psychodynamic therapy is ineffective for disruptive preschoolers, but studies of older children also suggest that psychodynamic treatments are not as effective as other treatments for disruptive behavior disorders ( 48 ). Research examining the effect of comorbid mood and anxiety problems on treatment outcomes may better inform decisions on whether to offer emotionally focused psychodynamic therapies for disruptive preschoolers.
Lessons from parent training interventions
Parent-oriented interventions are an important part of most day treatment programs, but the degree of parental involvement required varies among programs ( 1 ). The demonstrated efficacy of parent training programs in treating disruptive behavior disorders suggests that parent involvement in treatment programs should not be optional. Webster-Stratton and colleagues ( 27 , 29 ) have shown in two randomized controlled trials that parent training and child training have additive, perhaps synergistic, effects. The onus is on clinicians to find ways to engage parents of children in day treatment, even though parental stress and lack of resources may make these parents the most difficult to engage ( 11 ).
The results of the parent training studies suggest that programs that use active modeling of skills, audiovisual aids, and take-home materials have a better chance of maintaining parent participation. Video-based programs may engage families who are less verbal and facilitate generalization of concepts learned ( 49 ). Addressing parental stress in distressed families may also be crucial. It may be helpful to make participation more convenient for parents. Where resources allow, offering parent training in a variety of formats (individual, group, self-administered, and community based) may increase the likelihood of reaching more families ( 50 ).
Whether behaviorally oriented parent training and other family therapies have comparable effectiveness remains to be shown. In the meantime, introducing empirically supported parent training into existing multimodal day treatment programs may enhance the challenging work that clinicians do with families. However, family-oriented interventions that emphasize parental attunement and parental relationships (for example, parent-child interaction training and synthesis training) may be more acceptable to many practicing clinicians trained in psychodynamic or systemic methods. There is no evidence to suggest that behavioral and psychodynamic interventions cannot be delivered side by side. In the preschool day treatment program at Montreal's Institute of Community and Family Psychiatry, parents attend an Incredible Years parent training group and receive systemic and psychodynamic family therapy.
Lessons from classroom-based interventions
Social-learning principles likely guide interactions between teachers, therapists, and children in most day treatment programs. For example, reinforcement of positive behavior is present in many child programs in the form of sticker charts and other forms of token economies. A manualized program such as CLASS simply offers clinicians a systematic method of rewarding desired behaviors in a consistent fashion.
The efficacy of the Incredible Years teacher training program highlights the importance of the quality of classroom behavior management. Teachers and therapists in day treatment programs usually have formal training in child management, but booster courses and updates may be helpful. Again, video-based training and role plays may help teachers transfer learned skills into the classroom.
Conclusions
More research on the effectiveness of multimodal preschool day treatment programs is needed, both to ensure that children are receiving optimal treatment and to justify the cost of these programs. Randomized controlled trials comparing day treatment programs with less intensive outpatient treatments for disruptive preschoolers would be informative. Measuring multiple domains of functioning may be essential to represent gains that may be expected from a multimodal program, particularly as the comprehensive nature of day treatment may be one of its advantages.
In the absence of research on the optimal design of day treatment programs, clinicians can use evidence from laboratory-based intervention studies to inform practice. Specifically, the following elements of laboratory-based interventions may enhance day treatment.
• Provision of high-quality education
• Improved access to care for disadvantaged families via home visitation and transportation
• Attention to families' basic needs, including finances, health care, and nutrition
• Increased emphasis on children's social problem-solving skills
• Creative methods of delivering skills-oriented curricula, such as role play and puppetry
• Emphasis on parent training in behavior management
• Redoubled efforts to engage families in treatment by using multimedia programming, addressing parental stress, and offering treatment in more than one format
• Continued education for teachers and therapists.
More data on the effectiveness of laboratory-based interventions applied in clinical settings are needed to bridge the gap between laboratory-based and clinic-based research. Laboratory-based interventions can be tested in add-on studies in preschool day treatment programs. In addition, day treatment programs that have integrated novel interventions can report their outcomes. Research on the effectiveness and specific role of psychodynamic interventions is essential if they are to continue to be used in clinical programs.
Early childhood interventions may have long-term effects on the health of individuals and communities. It is important that clinicians continually examine and improve the interventions that they offer.
Acknowledgments
The author thanks Mark Zoccolillo, M.D., Carmella Roy, M.D., Ruth Russell, M.D., and Eric Fombonne, M.D., for their input and guidance.
1. Smolla N, Lebel A: Les centers de jour pedopsychiatriques pour la clientele des 0-12 ans au Quebec. [Child psychiatry day treatment centers for clients ages 0-12 in Quebec.]Revue Canadienne de Psychiatrie 43:714-721, 1998Google Scholar
2. Grizenko N: Outcome of multimodal day treatment for children with severe behavior problems: a five-year follow-up. Journal of the American Academy of Child and Adolescent Psychiatry 36:989-997, 1997Google Scholar
3. Richman N, Graham P, Stevenson J: Long-term effects of treatment in a pre-school day centre: a controlled study. British Journal of Psychiatry 142:71-77, 1983Google Scholar
4. Woollacott S, Graham P, Stevenson J: Controlled evaluation of the therapeutic effectiveness of a psychiatric day centre for pre-school children. British Journal of Psychiatry 132:349-355, 1978Google Scholar
5. McDermott BM, McKelvey R, Roberts L, et al: Severity of children's psychopathology and impairment and its relationship to treatment setting. Psychiatric Services 53:57-62, 2002Google Scholar
6. Ware LM, Novotny ES, Coyne L: A therapeutic nursery evaluation study. Bulletin of the Menninger Clinic 65:522-548, 2001Google Scholar
7. Baker BL, McIntyre LL, Blacher J, et al: Pre-school children with and without developmental delay: behavior problems and parenting stress over time. Journal of Intellectual Disability Research 47:217-230, 2003Google Scholar
8. Kaiser AP, Cai X, Hancock TB, et al: Teacher-reported behavior problems and language delays in boys and girls enrolled in Head Start. Behavior Disorders 28:23-29, 2002Google Scholar
9. Merrell KW, Holland ML: Social-emotional behavior of preschool-age children with and without developmental delays. Research in Developmental Disabilities 18:393-405,1997Google Scholar
10. Plomin R, Price TS, Eley TC, et al: Associations between behavior problems and verbal and nonverbal cognitive abilities and disabilities in early childhood. Journal of Child Psychology and Psychiatry 43:619-633, 2002Google Scholar
11. Cohen NJ, Bradley S, Kolers N: Outcome evaluation of a therapeutic day treatment program for delayed and disturbed preschoolers. Journal of the American Academy of Child and Adolescent Psychiatry 26:687-693, 1987Google Scholar
12. Weisz JR, Weiss B, Donenberg GR, et al: Bridging the gap between laboratory and clinic in child and adolescent psychotherapy. Journal of Consulting and Clinical Psychology 63:688-701, 1995Google Scholar
13. Kiser LJ, Pruitt DB, McColgan EB, et al: A survey of child and adolescent day-treatment programs: establishing definitions and standards. International Journal of Partial Hospitalization 3:247-259, 1986Google Scholar
14. Zimet SG: An American's perspective on day-treatment programs for children in France. International Journal of Partial Hospitalization 5:189-208, 1988Google Scholar
15. Kazdin AE: Evidence-based treatments: challenges and priorities for practice and research. Child and Adolescent Psychiatric Clinics of North America 13:923-940, 2004Google Scholar
16. Ollendick TH, King NJ: Empirically-supported treatments for children and adolescents: advances toward evidence-based practice, in Handbook of Interventions that Work With Children and Adolescents: Prevention and Treatment. Edited by Barrett PM, Ollendick TH. New York, Wiley, 2004Google Scholar
17. Culp RE, Little V, Letts D, et al: Maltreated children's self-concept: effects of a comprehensive treatment program. American Journal of Orthopsychiatry 61:114-121, 1991Google Scholar
18. Oates RK, Gray J, Schweitzer L, et al: A therapeutic preschool for abused children: the KEEPSAFE project. Child Abuse and Neglect 19:1379-1386, 1995Google Scholar
19. Johnson DL, Walker T: Primary prevention of behavior problems in Mexican-American children. American Journal of Community Psychology 15:375-385, 1987Google Scholar
20. Schweinhart LJ, Weikart DP, Larner MB: Consequences of three preschool curriculum models through age 15. Early Childhood Research Quarterly 1:15-45, 1986Google Scholar
21. Weikart DP: Changing early childhood development through educational intervention. Preventive Medicine 27:233-237, 1998Google Scholar
22. Raine A, Mellingen K, Liu J, et al: Effects of environmental enrichment at ages 3-5 years on schizotypal personality and antisocial behavior at ages 17 and 23 years. American Journal of Psychiatry 160:1627-1635, 2003Google Scholar
23. Rickel AU, Smith RL, Sharp KC: Description and evaluation of a preventive mental health program for preschoolers. Journal of Abnormal Child Psychology 7:101-112, 1979Google Scholar
24. Burke JD, Loeber R, Birmaher B: Oppositional defiant and conduct disorder: a review of the past 10 years, part II. Journal of the American Academy of Child and Adolescent Psychiatry 41:1275-1293, 2002Google Scholar
25. Reams R, Friedrich W: The efficacy of time-limited play therapy with maltreated preschoolers. Journal of Clinical Psychology 50:889-899, 1994Google Scholar
26. Shure MB, Spivack G: Interpersonal problem-solving in young children: a cognitive approach to prevention. American Journal of Community Psychology 10:341-356, 1982Google Scholar
27. Webster-Stratton C, Hammond M: Treating children with early-onset conduct problems: a comparison of child and parent training interventions. Journal of Consulting and Clinical Psychology 65:93-109, 1997Google Scholar
28. Webster-Stratton C, Reid MJ, Hammond M: Social skills and problem solving training for children with early-onset conduct problems: who benefits? Journal of Child Psychology and Psychiatry 42:943-952, 2001Google Scholar
29. Webster-Stratton C, Reid MJ, Hammond M: Treating children with early-onset conduct problems: intervention outcomes for parent, child, and teacher training. Journal of Clinical Child and Adolescent Psychology 33:105-124, 2004Google Scholar
30. Brestan EV, Eyberg SM: Effective psychosocial treatments of conduct-disordered children and adolescents: 29 years, 82 studies, and 5,272 kids. Journal of Clinical Child Psychology 27:180-189, 1998Google Scholar
31. Webster-Stratton C: Long-term follow-up of families with young conduct problem children: from preschool to grade school. Journal of Clinical Child Psychology 19:144-149, 1990Google Scholar
32. Forgatch MS, Toobert DJ: A cost-effective parent training program for use with normal preschool children. Journal of Pediatric Psychology 4:129-145, 1979Google Scholar
33. Hobbs SA, Forehand R: Effects of differential release from time-out on children's deviant behavior. Journal of Behavior Therapy and Experimental Psychiatry 6:256-257, 1975Google Scholar
34. Forgatch MS, DeGarmo DS: Parenting through change: an effective prevention program for single mothers. Journal of Consulting and Clinical Psychology 67:711-724, 1999Google Scholar
35. Webster-Stratton C, Hollinsworth T, Kolpacoff M: The long-term effectiveness and clinical significance of three cost-effective training programs for families with conduct-problem children. Journal of Consulting and Clinical Psychology 57:550-553, 1989Google Scholar
36. Taylor TK, Schmidt F, Pepler D, et al: A comparison of eclectic treatment with Webster-Stratton's Parent and Children Series in a children's mental health center: a randomized controlled trial. Behavior Therapy 29:221-240, 1998Google Scholar
37. Kazdin AE: Dropping out of child psychotherapy: issues for research and implications for practice. Clinical Child Psychology and Psychiatry 1:133-156, 1996Google Scholar
38. Schuhmann EM, Foote RC, Eyberg SM, et al: Efficacy of parent-child interaction therapy: interim report of a randomized trial with short-term maintenance. Journal of Clinical Child Psychology 27:34-45, 1998Google Scholar
39. Hood KK, Eyberg SM: Outcomes of parent-child interaction therapy: mothers' reports of maintenance three to six years after treatment. Journal of Clinical Child and Adolescent Psychology 32:419-429, 2003Google Scholar
40. Prinz RJ, Miller GE: Family-based treatment for childhood antisocial behavior: experimental influences on dropout and engagement. Journal of Consulting and Clinical Psychology 62:645-650, 1994Google Scholar
41. Wahler RG, Cartor PG, Fleischman J, et al: The impact of synthesis teaching and parent training with mothers of conduct disordered children. Journal of Abnormal Child Psychology 12:425-440, 1993Google Scholar
42. Dadds MR, Schwartz S, Sanders MR: Marital discord and treatment outcome in behavioral treatment of child conduct disorders. Journal of Consulting and Clinical Psychology 55:396-403, 1987Google Scholar
43. Sanders MR, Markie-Dadds C, Tully LA, et al: The Triple P Positive Parenting Program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. Journal of Consulting and Clinical Psychology 68:624-640, 2000Google Scholar
44. Webster-Stratton C: Advancing videotape parent training: a comparison study. Journal of Consulting and Clinical Psychology 62:583-593, 1994Google Scholar
45. Cunningham CE, Bremner R, Boyle M: Large group community-based parenting programs for families of preschoolers at risk for disruptive behavior disorders: utilization, cost effectiveness, and outcome. Journal of Child Psychology and Psychiatry 36:1141-1159, 1995Google Scholar
46. Walker HM, Kavanagh K, Stiller B, et al: First Step to Success: an early intervention approach for preventing school antisocial behavior. Journal of Emotional and Behavior Disorders 6:66-80, 1998Google Scholar
47. Kazdin AE, Siegel TC, Bass D: Drawing on clinical practice to inform research on child and adolescent psychotherapy: survey of practitioners. Professional Psychology: Research and Practice 21:189-198, 1990Google Scholar
48. Fonagy P, Target M, Cottrell D, et al: What Works for Whom? A Critical Review of Treatments for Children and Adolescents. New York, Guilford, 2002Google Scholar
49. Normandeau S, Venet M: Comment intervenir aupres et par l'entremise des parents [How to intervene with and through parents], in Prevention des Problemes d'Adaptation chez les Jeunes [Prevention of Problems of Adaptation Among Youth]. Edited by Vitaro F, Gagnon C. Quebec, Presses de l'Universite du Quebec, 2000Google Scholar
50. Webster-Stratton C, Taylor T: Nipping early risk factors in the bud: preventing substance abuse, delinquency, and violence in adolescence through interventions targeted at young children (0-8 years). Prevention Science 2:165-192, 2001Google Scholar

