
Public Knowledge, Beliefs, and Treatment Preferences Concerning Attention-Deficit Hyperactivity Disorder
Attention-deficit hyperactivity disorder (ADHD) and its treatment have sparked public and intellectual controversy for more than 40 years. Critics charge that ADHD is not a "real" disease but rather a constellation of behaviors that parents and schools have become unwilling or unable to tolerate. According to critics, parents and teachers accept diagnostic labels and psychostimulant prescriptions because they offer relatively straightforward, inexpensive, and fast-acting solutions to complex problems ( 1 , 2 , 3 , 4 ). By implication, critics claim that ADHD is overdiagnosed and that children are receiving unnecessary and inappropriate treatment.
Contrary to this claim, research on treatment utilization suggests that only half of children with ADHD receive treatment, and less than half of them receive specialty care ( 5 , 6 , 7 , 8 ). Fewer children receive psychostimulant medications than would be expected with estimated population prevalence rates ( 6 , 9 ), which supports the claim that ADHD is underdiagnosed and undertreated. The "International Consensus Statement on ADHD" ( 10 ) faults the media for publishing irresponsible stories that imply that ADHD is not a valid or real disorder. According to the statement, such stories diminish public recognition of the often devastating consequences of the disorder and the potential for medical treatments to alleviate them.
Given these competing discourses, it is important to understand the level of public awareness of ADHD and public preferences regarding its treatment. Such an understanding can offer insight into the degree to which the public accepts critical versus biomedical conceptualizations of the disorder. It also has the potential to explain observed differences in treatment utilization over time and across subgroups of the population ( 11 , 12 , 13 ). Growing public awareness of ADHD has been offered as one explanation for the expansion of treatment during the 1990s ( 11 ). Differences in knowledge about ADHD and in beliefs about the causes of the disorder also have been invoked to explain socioeconomic and racial and ethnic differences in treatment utilization ( 14 , 15 , 16 , 17 , 18 ).
What little we know about knowledge of and attitudes toward ADHD is based primarily on studies of school personnel and parents of children who are in treatment or are at risk of the disorder. Studies of school personnel suggest that teachers and school social workers are generally well informed about ADHD but that important knowledge gaps remain, particularly in regard to the role of diet as a cause of ADHD and the efficacy of behavioral interventions as stand-alone treatments ( 19 , 20 , 21 , 22 , 23 ). Studies of parents emphasize variations in beliefs about ADHD that are rooted in race and ethnicity. African-American parents are less likely than white parents to have heard of ADHD and to consider ADHD a medical problem, and they are more likely to attribute ADHD to excessive sugar in the child's diet ( 16 , 17 , 24 ).
In contrast, prior research provides little information about general public attitudes toward ADHD and its treatment. To our knowledge, the only study of general public attitudes compared responses to two vignettes: one in which a school-age boy's behavior problems were attributed to ADHD and a second in which the same set of behavior problems was attributed to epilepsy ( 25 ). Respondents were more accepting of medication therapies for the epileptic child than they were for the child with ADHD, indicating public resistance to medication use (and, perhaps, a biomedical conceptualization) for mental health problems.
In this article we present the results of a recent national survey concerned with public knowledge of and attitudes toward children's mental health problems. Our analysis extends prior research by investigating general knowledge and attitudes about ADHD, rather than relying on responses to vignettes, and by inquiring specifically about whether respondents believe that ADHD is "real" and about medication and counseling treatment options. The study considered general levels of public awareness and beliefs as well as variations by sociodemographic characteristics of the respondent: gender, race and ethnicity, education, income, and age.
We expected women's knowledge of and attitudes toward ADHD, in comparison with men's, to be more consistent with dominant psychiatric conceptualizations. Women generally are more predisposed than men to seek treatment for health problems ( 26 ) and are more likely to recognize and acknowledge psychiatric problems ( 27 ). Consistent with that expectation, fathers of sons with ADHD reported strong resistance to biomedical explanations and to medication strategies for treatment ( 28 ). We also expected to observe less knowledge about ADHD and less acceptance of biomedical understandings of the disorder among African Americans than among white respondents. We based this expectation on findings from research with parents of children at risk of ADHD ( 16 , 17 , 24 ) and studies that have found African Americans to be more skeptical about psychiatric medications and biomedical orientations to mental illness ( 29 , 30 ). Higher socioeconomic status, as indicated by years of education and income, was expected to predict greater awareness of ADHD and an endorsement of biomedically oriented treatments ( 31 ). We expected younger respondents to have more knowledge of ADHD than older respondents, because younger respondents grew up in a time when the disorder was more widely recognized.
Our models of treatment preferences also included as a predictor the belief that ADHD is real. Prior research suggests that beliefs about the nature of children's problems affect treatment decisions ( 7 , 16 ). We expected respondents who reported believing that ADHD is real to be more supportive of the use of medication for ADHD.
Methods
Participants
Data for the analysis come from the National Stigma Study-Children. All respondents to this module of the 2002 General Social Survey were asked a series of direct questions about ADHD and its treatment, which followed questions about a series of vignettes. Our analysis is based on the sample of respondents who had valid values on all of the variables (N=1,139). The sample used in this analysis was self-weighting. Institutional review board approval for the General Social Survey was provided by the University of Chicago, and approval for secondary data analysis was given by Indiana University.
Measures
To evaluate knowledge about ADHD, we first asked respondents, "Have you ever heard of attention-deficit hyperactivity disorder, or ADHD?" Respondents who answered yes were then asked, "Please tell me what you know about attention-deficit hyperactivity disorder, or ADHD." Respondents' answers to this second item were recorded verbatim by interviewers. We constructed two variables to measure knowledge of ADHD from these responses. The first variable indicated whether the respondent had ever heard of ADHD (yes, 1; no, 0); the responses of 16 persons who answered yes to the first question but who were unable to say anything about ADHD in response to the follow-up item were recoded as "no" responses. The second variable represented the content of the open-ended responses to the second question. Two research assistants independently coded the open-ended responses and reconciled the few discrepancies through consultation. Only one response was coded for each respondent, in keeping with the brevity of most answers.
Respondents who said they had heard of ADHD were asked three yes-no questions, which we used to indicate beliefs and treatment preferences. The first was, "Do you think ADHD is a real disease?" Responses were coded 1 for yes or 0 for no. This question was intended to tap whether the respondents accepted a biomedical conceptualization of the disorder. The second and third questions were, "Should children be given counseling for ADHD?" and "Should children be given medication to treat ADHD?" These two variables were used to construct a single categorical variable for whether the respondent felt children should be given counseling only, medication only, both treatments, or neither treatment.
The analysis considered five sociodemographic characteristics as predictors of the outcome measures. These were binary variables for gender (men, 1; women, 0) and race (African Americans, where African Americans were coded 1 and whites and others were coded 0, and other races, where respondents of other races were coded 1 and white respondents and African Americans were coded 0) and continuous variables for age, measured in years; annual family income, measured in thousands of dollars; and education, measured in years of schooling completed.
Data analysis
We present descriptive statistics for respondents' awareness of ADHD, their open-ended responses to what they knew about ADHD, their evaluation of whether ADHD is a "real disease," and their treatment preferences. We used binary logistic regression models to evaluate the associations between respondents' sociodemographic characteristics, having heard of ADHD, and the belief that ADHD is a real disease. We used multinomial logistic regression models for the comparable set of analyses to predict the content of respondents' knowledge about ADHD and their treatment preferences. Multinomial logistic regression models extend the logic of binary logistic regression to the case where the dependent variable has more than two values. All reported significance tests were two-tailed.
Results
Knowledge of ADHD
Table 1 presents the distributions for awareness of ADHD and the content of respondents' knowledge. Not quite two-thirds of General Social Survey respondents (64%) indicated that they had heard of ADHD and were able to provide an answer when asked what they knew.
 |
Responses varied in terms of content and degree of sophistication. The most common response, given by almost one-third of respondents, described symptoms (such as impulsive or hyperactive) that are consistent with clinically established consensus. Other respondents mentioned medication or chemical or biological causes that reflect biomedical understandings of the disorder. The next most common categories of response included generalizations that indicated limited knowledge of the disorder (such as "I have heard of it") or names of people (including themselves) who "had it" or "have it." Roughly 13% of respondents gave other types of responses, the most common of which were negative sentiments about the use of medications or the diagnosis of ADHD in line with critics' claims (such as "ADHD isn't real"). In summary, even among respondents who said that they had heard of ADHD, most were not able to describe specific content knowledge.
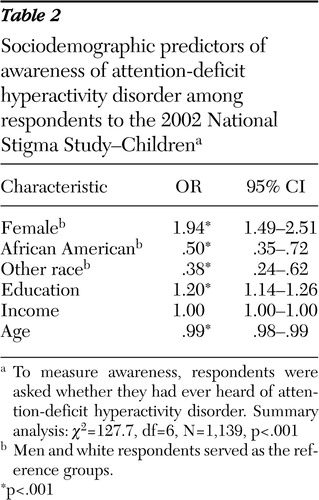
Knowledge of ADHD varied systematically with respondents' sociodemographic characteristics. Odds ratios and 95% confidence intervals from the logistic regression on the sociodemographic variables for having heard of ADHD are given in Table 2 . Women were more likely than men to say that they had heard of ADHD, as were respondents with higher levels of education. African Americans, members of other nonwhite racial and ethnic groups, and older respondents were less likely to say that they had heard of ADHD. After the analyses controlled for the other sociodemographic characteristics, income did not predict knowledge of ADHD.
 |
In supplementary analyses, we evaluated whether there were significant sociodemographic differences in the content of respondents' knowledge about ADHD (results available on request). To do so, we estimated multinomial logistic regression models that predicted knowledge content from respondents' sociodemographic characteristics. For purposes of this analysis, we combined the open-ended responses described above into six more general thematic categories: symptoms, medication and chemical causes, awareness ("heard of it"), knew someone with ADHD, anti-ADHD sentiments, and other responses.
There were few significant sociodemographic differences in knowledge content, and those few did not follow a consistent pattern. Specifically, there were no significant differences in content knowledge by gender or income. There were a few scattered but inconsistent differences by race and education. African Americans were less likely than white respondents to mention knowing someone with ADHD than they were to give another answer. The same was true for respondents with higher levels of education. The only consistent pattern was that older respondents were more likely than younger respondents to have heard of ADHD or to give a response categorized as "other" than they were to describe symptoms, mention medication or chemical causes, or express overt anti-ADHD sentiments. This finding suggests that older respondents had less specific knowledge of the disorder than younger respondents. Results from multinomial logistic regression models that predicted broader content categories—specific knowledge, nonspecific knowledge, and other responses—were similar.
The belief that ADHD is real
Of respondents who had heard of ADHD, over three-quarters (78%) reported believing that it is a "real disease." Belief in the reality of ADHD varied with the content of respondents' knowledge. Table 3 presents the percentage of respondents in each of the six major knowledge content categories who reported believing that ADHD is real. Respondents who said they knew someone with ADHD were most likely to say that ADHD was real, followed closely by respondents who described symptoms, who mentioned medication or chemical causes, and those who had simply heard of it. Respondents who expressed anti-ADHD sentiments or who gave other responses (that the disorder is rooted in primarily social, environmental, or diet-based causes) were least likely to say that ADHD was real. The belief that ADHD is real varied significantly across the thematic categories ( χ2 =34.29, df=5, p<.001).
 |
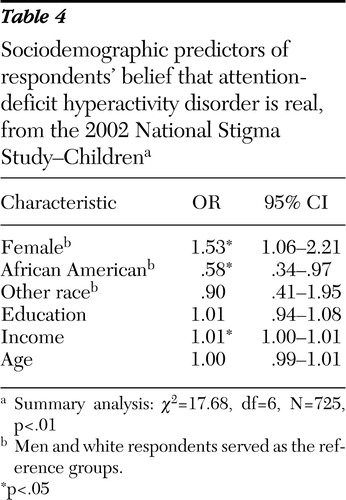
The odds ratios and 95% confidence intervals for the logistic regression on respondents' sociodemographic characteristics of their belief that ADHD is real are given in Table 4 . Women were more likely than men to believe that ADHD is real, as were people with higher levels of income. African Americans were less likely than white respondents to say that ADHD is real. The likelihood of believing that ADHD is real did not differ between white respondents and members of other racial and ethnic groups, by education, or by age.
 |
Treatment preferences
The last part of our analysis evaluated treatment preferences for ADHD. Table 5 presents the frequencies for respondents' preferences for counseling, medication, both, or neither. Most respondents reported believing that children with ADHD should be given a combination of counseling and medication, consistent with professional recommendations. Of those who preferred only one treatment approach, however, almost four times as many expressed a preference for counseling as for medication. Only a small percentage of respondents felt that children with ADHD should receive neither counseling nor medication.
 |
Treatment preferences were only weakly associated with sociodemographic characteristics but were strongly associated with respondents' beliefs about whether ADHD is real. Using a strategy similar to our analysis of content knowledge, we estimated a multinomial logistic regression that predicted the four-category treatment preference variable from the six sociodemographic variables and from the belief that ADHD is real (results available on request).
No significant differences in treatment preferences were based on education or income, and few differences were associated with the other sociodemographic characteristics. Men were more likely than women to endorse no treatment rather than a combined treatment approach, but men and women did not differ in their preferences for counseling or medication alone. African Americans were more likely than white respondents to prefer counseling or a combined counseling-medication approach over no treatment. Older respondents were more likely than younger respondents to prefer a combined treatment approach over counseling or no treatment. With those few exceptions, there were no other sociodemographic differences in treatment preferences. The most consistent differences involved the belief that ADHD is real. Respondents who said they believed ADHD is real were more likely to prefer any form of treatment—a combined treatment approach, counseling alone, or medication alone—over no treatment.
Discussion
This study described public knowledge about ADHD and preferences for its treatment. Taken together, the results suggest that the public is not well informed about the disorder or its treatment, at least as the disorder is defined by the psychiatric profession. Only about two-thirds of respondents said they had heard of ADHD, and when asked to say what they knew, fewer than half gave a specific answer that was consistent with the dominant psychiatric conceptualization of the disorder. Moreover, although most respondents supported counseling and medication as appropriate treatments for ADHD, many fewer supported medications than supported counseling, and almost 10% supported neither approach.
The questions with which we assessed content knowledge of ADHD relied on respondents' abilities to articulate what they knew about ADHD to the interviewer. It is possible that we would have observed a higher level of knowledge if we had offered respondents a checklist of items with which to agree or disagree rather than depending on spontaneous reports. That having been said, spontaneous reports offered important insight into the knowledge that respondents were able to express about ADHD.
The question regarding whether ADHD is real was intended to capture acceptance of biomedical understandings of the disorder. However, the word "real" may have been interpreted differently by different respondents. This possibility raises questions about the most appropriate interpretation of our results. The belief that ADHD is real was more common among respondents who described the symptoms of the disorder and was less common among respondents who described ADHD as having social, environmental, or dietary causes and among those with an anti-ADHD stance. These patterns suggest that believing ADHD is real is, as intended, partly about accepting biomedical understandings. However, belief that ADHD is real was also more common among respondents who knew someone with the disorder, which suggests that the word "real" also implies legitimacy—that the person has a "real" problem that merits attention. The latter interpretation was confirmed by the results of our analysis of treatment preferences. Belief that ADHD is real predicted preference for some type of treatment over no treatment and for medication over counseling, independent of respondents' sociodemographic characteristics.
Sociodemographic differences in knowledge about ADHD and in the belief that ADHD is real were generally consistent with our expectations. The strongest and most consistent differences were for gender, race and ethnicity, and age. As we expected, women were more likely than men, and African Americans were less likely than white respondents, to have heard of ADHD and to believe that ADHD is real. Older respondents were also less likely to have heard of ADHD and had less specific knowledge of the disorder. However, there were few consistent differences in treatment preferences that were based on respondents' sociodemographic characteristics. Among persons who had heard of ADHD, there was widespread endorsement of counseling and of combined treatment approaches across all groups.
With respect to treatment preferences, our analysis revealed lingering skepticism over medication treatments. In a study based on data from the 1998 General Social Survey, McLeod and colleagues ( 32 ) reported that only about 30% of respondents said they were very willing or somewhat willing to give medication to a child who had symptoms consistent with a diagnosis of ADHD. Similar skepticism about medications was evident in this study, particularly as a sole treatment. Whereas few respondents thought children with ADHD should not receive treatment, many more respondents expressed a preference for combined treatment or for counseling alone over medications alone.
Conclusions
Our findings point to a critical need to educate the public about the symptoms of ADHD, its causes, and the treatments that have proven effective. Although media and educational efforts should make a special effort to reach populations such as African Americans and older respondents, who have less specific knowledge about the disorder, we emphasize that respondents' treatment preferences were only weakly related to sociodemographic characteristics. They stand in stark contrast to evidence from carefully controlled clinical trials, such as the Multimodal Treatment Study of ADHD trials ( 33 , 34 , 35 , 36 ), which indicate that medication is substantially more efficacious than even the most intensive forms of therapy or counseling for children without significant comorbidities.
This study represents only a first step toward addressing Conrad and Potter's ( 37 ) call to understand more fully "how medical diagnoses penetrate the public consciousness." The questions analyzed here pertain to general awareness and beliefs about ADHD, rather than about the conditions under which respondents would recognize symptoms of ADHD or react to children who meet clinical criteria, whether as their caregivers or as community members. Future research should be oriented to answering more nuanced questions about public perceptions of ADHD.
Acknowledgments and disclosures
The authors acknowledge project support by the National Science Foundation to the National Opinion Research Center; Eli Lilly and Company; the Office of the Vice President for Research, Indiana University; and grant K02-MH-012989 from the National Institutes of Health and National Institute of Mental Health to Dr. Pescosolido, principal investigator. Partial support for the analyses was provided by grant R01-HD-050288 from the National Institute of Child Health and Human Development to Dr. McLeod. The authors thank Tom Smith and staff members of the Indiana Consortium for Mental Health Services Research, Schuessler Institute for Social Research, Indiana University.
The authors report no competing interests.
1. DeGrandpre RJ: Ritalin Nation. New York, Norton, 1999Google Scholar
2. Schlesinger M, Gray BH, Perreira KM: Medical professionalism under managed care: the pros and cons of utilization review. Health Affairs 16(1):106–124, 1997Google Scholar
3. Breggin PR: Talking Back to Ritalin. Monroe, Maine, Common Courage Press, 1998Google Scholar
4. Diller L: The run on Ritalin: attention deficit disorder and stimulant treatment in the 1990s. Hastings Center Report 26:12–18, 1996Google Scholar
5. Bauermeister JJ, Canino G, Bravo M, et al: Stimulant and psychosocial treatment of ADHD in Latino/Hispanic children. Journal of the American Academy of Child and Adolescent Psychiatry 42:851–855, 2003Google Scholar
6. Canino G, Shrout PE, Rubio-Stipec M, et al: The DSM-IV rates of child and adolescent disorders in Puerto Rico. Archives of General Psychiatry 61:85–93, 2004Google Scholar
7. Jensen PS, Bhatara V, Vietello B, et al: Psychoactive medication prescribing practices for US children: gaps between research and clinical practice. Journal of the American Academy of Child and Adolescent Psychiatry 38:557–565, 1999Google Scholar
8. Jensen P: Closing the evidence-based treatment gap for children's mental health services: what we know vs what we do. Emotional and Behavioral Disorders in Youth 2:43–50, 2002Google Scholar
9. Goldman LS, Genel M, Bezman RJ, et al: Diagnosis and treatment of attention-deficit/hyperactivity disorder in children and adolescents. JAMA 279:1100–1107, 1998Google Scholar
10. Barkley RA, Cook EH, Diamond A, et al: International Consensus Statement on ADHD. Clinical Child and Family Psychology Review 5:89–111, 2002Google Scholar
11. Olfson M, Gameroff MJ, Marcus SC, et al: National trends in the treatment of attention deficit hyperactivity disorder. American Journal of Psychiatry 160:1071–1077, 2003Google Scholar
12. Jorm AF: Mental health literacy: public knowledge and beliefs about mental disorders. British Journal of Psychiatry 177:396–401, 2000Google Scholar
13. DosReis S, Zito JM, Safer D, et al: Parental perceptions and satisfaction with stimulant medication for attention-deficit hyperactivity disorder. Journal of Developmental and Behavioral Pediatrics 24:155–162, 2003Google Scholar
14. Goodwin R, Gould MS, Blanco C, et al: Prescription of psychotropic medications to youths in office-based practice. Psychiatric Services 52:1081–1087, 2001Google Scholar
15. Leslie LK, Weckerly J, Landsverk J, et al: Racial-ethnic differences in the use of psychotropic medication in high-risk children and adolescents. Journal of the American Academy of Child and Adolescent Psychiatry 42:1433–1442, 2003Google Scholar
16. Bussing R, Schoenberg NE, Rogers KM, et al: Explanatory models of ADHD: do they differ by ethnicity, child gender, or treatment status? Journal of Emotional and Behavioral Disorders 6:233–243, 1998Google Scholar
17. Yeh M, Hough RL, McCabe K, et al: Parental beliefs about the causes of child problems: exploring racial/ethnic patterns. Journal of the American Academy of Child and Adolescent Psychiatry 43:605–612, 2004Google Scholar
18. Bussing R, Gary FA, Mills TL, et al: Parental explanatory models of ADHD: gender and cultural variations. Social Psychiatry and Psychiatric Epidemiology 38:563–575, 2003Google Scholar
19. Kos JM, Richdale AL, Hay DA: Children with attention deficit hyperactivity disorder and their teachers: a review of the literature. International Journal of Disability, Development, and Education 53:147–160, 2006Google Scholar
20. Cornell-Swanson L, Irwin M, Johnson K, et al: The use of stimulant medication for treatment of attention-deficit/hyperactivity disorder: A survey of school social workers' knowledge, opinions/attitudes, and experience. School Social Work Journal 29:62–82, 2005Google Scholar
21. Bekle B: Knowledge and attitudes about attention-deficit hyperactivity disorder (ADHD): a comparison between practicing teachers and undergraduate education students. Journal of Attention Disorders 7:151–161, 2004Google Scholar
22. Frankenberger W, Farmer C, Parker L, et al: The use of stimulant medication for treatment of attention-deficit/hyperactivity disorder: a survey of school psychologists' knowledge, attitudes, and experience. Developmental Disabilities Bulletin 29:132–151, 2001Google Scholar
23. Jerome L, Washington P, Laine CJ, et al: Graduating teachers' knowledge and attitudes about attention-deficit hyperactivity disorder: a comparison with practicing teachers. Canadian Journal of Psychiatry 44:192, 1999Google Scholar
24. Bussing R, Schoenfeld N, Perwien ER: Knowledge and information about ADHD: evidence of cultural differences among African American and white parents. Social Science in Medicine 46:919–928, 1998Google Scholar
25. Summers JA, Caplan PJ: Laypeople's attitudes toward drug treatment for behavioral control depend on which disorder and which drug. Clinical Pediatrics 26:258–263, 1987Google Scholar
26. Waldron I: Gender and health-related behavior, in Health Behavior: Emerging Research Perspectives. Edited by Gochman DS. New York, Plenum Press, 1995Google Scholar
27. Horwitz AV: The pathways into psychiatric treatment: some differences between men and women. Journal of Health and Social Behavior 18:169–178, 1977Google Scholar
28. Singh I: Boys will be boys: fathers' perspectives on ADHD symptoms, diagnosis, and drug treatment. Harvard Review of Psychiatry 11:308–316, 2003Google Scholar
29. Schnittker J: Misgivings of medicine? African Americans' skepticism of psychiatric medication. Journal of Health and Social Behavior 44:506–525, 2003Google Scholar
30. Schnittker J, Freese J, Powell B: Nature, nurture, neither, nor: black-white differences in beliefs about the causes and appropriate treatment of mental illness. Social Forces 78:1101–1130, 2000Google Scholar
31. Schnittker J, Pescosolido BA, Croghan TW: Are African Americans really less willing to use health care? Social Problems 52:255–271, 2005Google Scholar
32. McLeod JD, Pescosolido BA, Takeuchi DT, et al: Public attitudes toward the use of psychiatric medications for children. Journal of Health and Social Behavior 45:53–67, 2004Google Scholar
33. The MTA Cooperative Group: Moderators and mediators of treatment response for children with attention-deficit/hyperactivity disorder. Archives of General Psychiatry 56:1088–1096, 1999Google Scholar
34. The MTA Cooperative Group: A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry 56:1073–1086, 1999Google Scholar
35. The MTA Cooperative Group: National Institute of Mental Health Multimodal Treatment Study of ADHD follow-up: changes in effectiveness and growth after the end of treatment. Pediatrics 113:762–769, 2004Google Scholar
36. The MTA Cooperative Group: National Institute of Mental Health Multimodal Treatment Study of ADHD follow-up: 24-month outcomes of treatment strategies for attention-deficit/hyperactivity disorder. Pediatrics 113:754–761, 2004Google Scholar
37. Conrad P, Potter D: From hyperactive children to ADHD adults: observations on the expansion of medical categories, in Health and Health Care as Social Problems. Edited by Conrad P, Leiter V. Lanham, Md, Rowman and Littlefield, 2003Google Scholar

