
Employment Among Persons With Past and Current Mood and Anxiety Disorders in the Israel National Health Survey
Common mental disorders are prevalent among working people ( 1 , 2 , 3 , 4 , 5 , 6 ) and are known to have a disabling effect and to lower productivity ( 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 ). Previous studies have examined whether recovery from an episode of depression was followed by improved job performance ( 10 , 15 , 16 ). Patients with more favorable depression outcomes showed significant improvement in their job performance ( 10 , 16 ). However, one study found that this improvement was consistently worse than improvement in two comparison groups—individuals with rheumatoid arthritis and individuals without depression ( 10 ).
Because of the expected lifetime prevalence of common mental disorders in Israel ( 17 ) and the known effects on employment of these disorders, it is important to investigate this question at the national level. The study reported here sought to determine whether the results described above, which were obtained from carefully designed, small follow-up studies, could be replicated in an analysis of data from a large epidemiological survey. The study used data from a nationally representative community health survey in Israel to compare work participation, salary, and self-reported reasons for unemployment in four groups of survey respondents: those with a past-month diagnosis of a mood or anxiety disorder, those with a past-year diagnosis of a mood or anxiety disorder who did not have a disorder in the past month, those with lifetime a diagnosis of a mood or anxiety disorder who did not have a disorder in the past year, and those with no diagnosis of a mood or anxiety disorder.
Methods
The Israel National Health Survey followed procedures established by the World Mental Health Survey (WMH) of the World Health Organization (WHO) ( 18 ). The sample was extracted from Israel's National Population Register and comprised noninstitutionalized legal residents aged 21 and over. The sample was designed to reflect the population distribution by age, gender, and three population sectors: Arabs; post-1990 Jewish immigrants from the former Soviet Union; and Jews and others, including Jewish immigrants from countries other than the former Soviet Union. The sample interviewed for the Israel National Health Survey was weighted back to the total population to compensate for unequal selection probabilities resulting from disproportionate stratification, clustering effects, and nonresponse. The weights were adjusted to make sample totals conform to known population totals taken from reliable Central Bureau of Statistics sources.
On first personal contact with each potential survey respondent, the interviewer explained the survey and obtained verbal informed consent ( 19 ). Overall, 73% of those contacted agreed to be interviewed (88% of Arab-Israelis and 71% of Jewish-Israelis). If a person refused to participate, no replacement was made. A total of 4,859 face-to-face interviews were conducted in Arabic, Hebrew, or Russian at respondents' homes from May 2003 to April 2004. Professional survey interviewers, who were trained and supervised by the Central Bureau of Statistics, used a laptop computer and computer-assisted personal interview methods. Interviews lasted an average of 60 minutes. The Human Subjects Committee at Eitanim-Kfar Shaul Hospital approved the survey and the field procedures in November 2000.
Measures
The analyses presented here are based on the following sections of the interview schedule.
Diagnostic assessment. The diagnostic instrument used in the WHO-WMH was the Composite International Diagnostic Interview (CIDI) ( 18 ), a fully structured diagnostic instrument that assesses lifetime and recent prevalence of selected psychiatric disorders according to both ICD-10 and DSM-IV diagnoses. The Israel survey assessed for anxiety disorders (panic disorder, generalized anxiety disorder, agoraphobia without panic disorder, and posttraumatic stress disorder), mood disorders (major depressive disorder, dysthymia, and bipolar I and II disorders), and substance use disorders. The presence of a disorder was determined by whether respondents' past or current symptoms met 12-month or lifetime diagnostic criteria for a DSM-IV disorder. For each disorder, a screening section was administered to the respondent. When a respondent endorsed a specific screening item, he or she was asked all the questions in the CIDI diagnostic section for that disorder to establish the presence of a current disorder. Persons who reported the presence of an organic disorder that accounted for their symptoms were not included in the sample.
The validity of the WHO-WMH CIDI as a diagnostic tool was assessed in France, Italy, Spain, and the United States by a clinical reappraisal study ( 20 ). That study sought to determine whether CIDI diagnoses were consistent with those obtained independently by trained clinicians who administered the Structured Clinical Interview for DSM-IV (SCID) to a subsample of survey respondents who had previously completed the CIDI. The individual-level concordance between the SCID and CIDI for 12-month prevalence of any mood disorder, any anxiety disorder, and any disorder overall was substantial (area under the curve in the range of .8 to .9) ( 20 ).
For the analyses reported here, respondents were grouped into those with or without any mood or anxiety disorder, because one-third of those with any anxiety disorder also had a mood disorder. All respondents with a 12-month alcohol or drug use disorder had a comorbid anxiety or mood disorder and were therefore included in the anxiety or mood disorder group. The analysis distinguished between four groups of respondents in terms of a mood or anxiety disorder: those with no disorder, those with a lifetime disorder but no disorder in the past 12 months, those with a 12-month disorder but no disorder in the past 30 days, and those with a disorder in the past 30 days.
Age at onset. The survey included an item on age at onset: "How old were you the first time you had the symptoms?" Respondents who could not remember were asked whether onset was before they started school, before their teens, or later. Age at onset, a continuous variable, was divided into two categories of equal size: aged 24 and younger and aged 25 and older. The multivariate analysis used three categories: no age at onset (no disorder), onset at 24 or younger, and onset at 25 or older.
Chronic general medical conditions. The survey included a checklist of chronic general medical disorders and chronic pain. The conditions listed were heart attack, heart disease, stroke, high blood pressure, asthma, chronic obstructive pulmonary disorder, emphysema or other lung disease, tuberculosis, diabetes, kidney disease, neurological conditions, thyroid disease, cancer, chronic back or neck pain, arthritis or rheumatism, headaches, or any other chronic pain. Respondents were asked whether they ever experienced any of the symptoms of these conditions and, if so, whether they experienced them at any time in the past 12 months. For conditions that are typically identified by medical diagnosis, such as heart disease, respondents were asked whether a doctor or other health professional had ever told them that they had the condition, and if so, whether they had the condition in the past 12 months. The question about the past 12 months was omitted for conditions that persist throughout the life course. In this analysis, respondents with chronic general medical conditions were grouped into a two categories: those reporting any one of the conditions and those reporting none.
Methodological research has shown that such checklists provide useful information about treated or currently untreated chronic conditions ( 21 ) and that they predict use of outpatient health care, hospitalization, and mortality ( 22 ). Such research has also shown that self-report of chronic general medical conditions is in moderate to high agreement with medical records data ( 23 ).
Service use for emotional or mental problems. Respondents were asked whether they had ever visited any of a list of professionals to talk about problems related to their mental or emotional health. The professionals listed were specialist mental health service providers (such as psychologists, psychiatrists, and social workers), general medical professionals (such as general practitioners), religious counselors (such as rabbis and sheikhs), and healers (such as naturopaths).
Employment, monthly salary, and occupation. All survey respondents were asked to report their salary in the previous month. For the study reported here, respondents' reports of employment and income for the previous month were used. Income was then categorized into two groups: above and below the average monthly salary in Israel (about $1,500 U.S. dollars at the time of the study).
All respondents were asked to describe the type of work they did in their place of work. The answers were classified by Central Bureau of Statistics staff into ten occupational groups on the basis of the International Labour Organization's Classification of Occupations ( 24 ). For this study the ten classes of occupations were categorized into three groups: professionals and managers, skilled workers, and unskilled workers.
Employment restrictions. All respondents were asked about whether they had physical or emotional problems that placed limits on employment and whether they were out of the workforce, temporarily unemployed, or employed full-time. The following three questions were used in this study: "Are you limited in the kind or amount of work you can do because of problems with your physical or emotional health?" "What is the main reason you are not working and also not looking for a job?" "Do you have any problems with your physical or emotional health that would prevent you from working for pay if you wanted to?" Four mutually exclusive categories were used for restriction: due to general medical problems, due to mental health problems, due to both general medical and mental health problems, and no health restrictions on employment. Respondents who stated that they did not work or were not looking for work because they had retired or were homemakers or who stated a reason other than health were classified as having no health restrictions on employment.
Statistical analysis
The data were weighted to adjust for the differential probabilities of respondents' selection and nonresponse and for differences between the sample and the adult population in Israel. Prevalence rates in the four disorder status groups (none, lifetime, past year, and past month) were calculated by gender, age, and the three population groups on the basis of weighted data, along with estimates of standard errors.
Logistic regression analyses were conducted with SUDAAN ( 25 ) to estimate the association between being employed and mental disorder status in the entire sample adjusted for age, gender, and any chronic general medical condition; the association between being employed and disorder status among respondents with any mental disorder adjusted for age, gender, education, any chronic general medical condition, and any past treatment for mental problems; and the association between being in the higher-than-average salary group and disorder status among those who were working in the previous month adjusted for age, gender, education, and age at onset of mental problems.
Another set of regression analyses was conducted for respondents who were unemployed or who had employment limitations in order to estimate the association between the reported reason for lack of employment and mental disorder status adjusted for age, gender, education, and any chronic general medical condition. The logistic regression coefficients were transformed to odds ratios (ORs) and 95% confidence intervals (CIs).
Results
Disorder status by gender, age, and population group
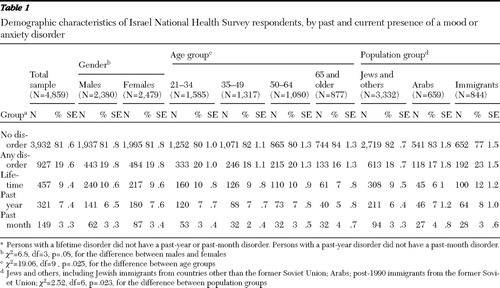
Table 1 shows the composition by subgroup—gender, age, and population sector—of the four mental disorder status groups. Lifetime prevalence of a mood or anxiety disorder was 19% for the entire sample, as it was for most of the subgroups except for respondents aged 65 and older (16%) and immigrants (23%). The rates for these two groups were significantly different from those in the other groups and in the sample overall. Past-month prevalence of a mood or anxiety disorder was 3% for the overall sample, as it was for most of the subgroups except for those aged 65 and older (4%) and Arabs (4%). These rates were not significantly different.
 |
Disorder status and employment
Table 2 shows the proportions of respondents who reported employment in the month before the interview, by age and mental disorder status. Employment was significantly related to the presence of a mental disorder in all age groups except the youngest group. Those who reported a mood or anxiety disorder in the previous month had the lowest rates of employment, whereas the employment rates of those with a lifetime or past-year mood or anxiety disorder did not differ from the rates of respondents who reported no disorder. For example, in the 35- to 49-year age group, the employment rate among those with a past-month mood or anxiety disorder was 35%, compared with rates of 74%, 77%, and 58%, respectively, among those who had no disorder, who had a lifetime disorder, and who had a past-year disorder.
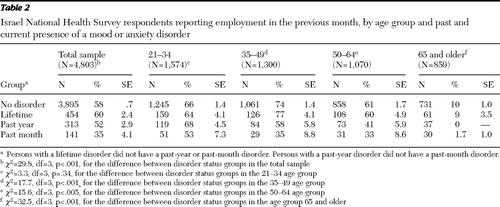 |
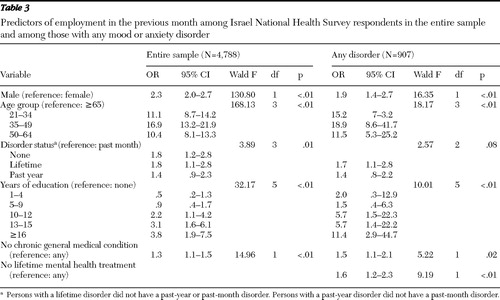
Table 3 presents data on the likelihood of being employed in the past month among persons in the entire sample and among survey respondents who reported any mood or anxiety disorder (lifetime, past year, or past month). The odds were adjusted for mental disorder status group, gender, age group, years of education, and the presence of any general medical condition. In the entire sample, the odds of being employed were the same for the group with no disorder and the group with a lifetime disorder (OR=1.8 for both); these odds were significantly higher than the odds of being employed among those with a past-month disorder (reference group). Among those with a disorder in the previous year, the odds of being employed (OR=1.4) were not significantly different from the odds in the past-month disorder group. In the analysis shown in Table 3 that examined the odds of being employed only among respondents who reported any mood or anxiety disorder, the results were similar. This model included an additional variable—lifetime receipt of some form of treatment for mental health problems. The odds of being employed were higher among respondents who reported no use of any services for mental health problems.
 |
Disorder status and salary
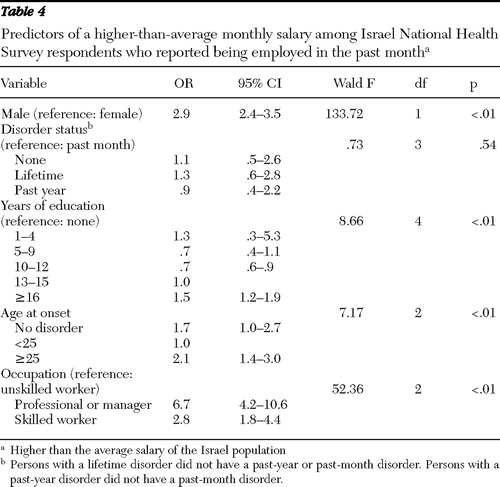
Table 4 shows the odds of being in the higher-than-average salary group for respondents who worked in the past month. After the analysis adjusted for gender, mental disorder status group, education, and type of occupation, earning an above-average salary was found to be a function of age at onset of the disorder. Respondents whose first episode of anxiety or depression occurred at age 25 or older had twice the odds of earning an above-average salary as those whose first episode occurred at age 24 or younger (reference group), regardless of whether they reported a disorder in the past month, the past year, or at an earlier time. The percentage of respondents earning an above-average salary was higher in the later-onset group than in the earlier-onset group (33.1%±3.1% compared with 23.8%±2.3%; χ2 =14.2, df=1, p<.001). The percentages of respondents earning a higher salary did not differ significantly by occupational group or mental disorder status group.
 |
Differences between population groups
Two analyses were conducted to determine whether adding the variable for population group (Arabs; post-1990 immigrants from the former Soviet Union; and Jews and others, including Jewish immigrants from countries other than the former Soviet Union) changed the results in terms of prediction of past-month employment or above-average salary. Population group was a significant predictor of employment and salary in both analyses, but adding it did not change the main results—that is, the significance of past-month disorder status and age at onset as predictors. In an analysis that adjusted for population group, gender, and age group and used the group with a past-month mood or anxiety disorder as the reference group (OR=1), the odds of being employed were significantly higher in the group with a past-year disorder (OR=1.9, CI=1.1–2.9) as well as in the group with a lifetime disorder (OR=2.6, CI=1.6–2.4). Similarly, in an analysis that adjusted for population group, gender, age at onset, and occupation and used the group with onset before age 25 as the reference group (OR=1), the odds of having a higher-than-average salary were significantly greater among those with a later onset of illness (OR=2.0, CI=1.4–3.0).
Reasons for limits on employment
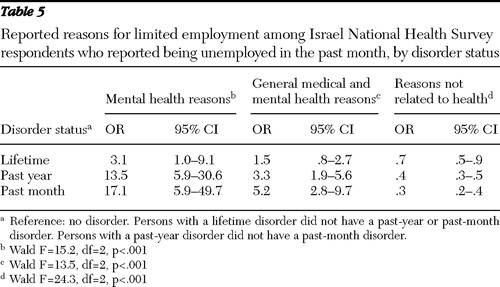
Respondents who did not work in the month before the interview gave reasons for their unemployment ( Table 5 ). An analysis that adjusted for age, education, any chronic general medical condition, and gender was conducted to examine three reasons—mental health problems, general medical and mental health problems, and no health problems—among the mental disorder status groups. When the reference group was unemployed respondents who never had a mood or anxiety disorder (OR=1.0), respondents with a lifetime disorder had significantly higher odds of citing mental health reasons (OR=3.1), and the odds were even greater among those with a past-year disorder (OR=13.5) and a past-month disorder (OR=17.1). In a similar analysis with the same reference group, the odds of citing general medical and mental health problems were significantly higher among those with a past-year disorder (OR=3.3) and a past-month disorder (OR=5.2,) and the odds of not citing a health problem as a reason for unemployment were significantly lower among those with a lifetime disorder (OR=.3), those with a past-year disorder (OR=.4), and those with a past-month disorder (OR=.7).
 |
Discussion
Data from the Israel National Health Survey, which used a representative sample of the adult population of Israel, were examined to identify differences in employment and earnings among respondents with a lifetime mood or anxiety disorder who had been in remission for at least one year and those with a disorder in the past year or the past month. The results replicate previous findings showing lower employment rates among persons in the acute phase of a common mental disorder ( 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 ).
The study reported here, however, also showed that employment among persons who recovered from an episode of a mood or anxiety disorder could return to a rate similar to rates found for respondents who had never had an anxiety or depressive disorder. Both those with a lifetime disorder and those with a past-year disorder were more likely to be employed than those with a past-month disorder. Rates of employment in the survey were based on past-month employment only and did not necessarily reflect rates of long-term employment. Also, rates of employment among those with a lifetime or past-year disorder may reflect a tendency to continue to work despite a possible reduction in productivity ( 26 ).
Among survey respondents with a lifetime disorder but no disorder in the past year or the past month, the odds of being employed for those who reported receipt of any type of treatment for mental health problems were lower than for those who reported receiving no treatment. We assume that this unexpected result reflects the fact that, in general, individuals with more severe disorders are more likely to seek help—as is the case in Israel ( 27 )—and less likely to be employed. Thus, after the analysis controlled for severity (indicated by any receipt of treatment), the odds of being employed were higher for those with a lifetime or past-year disorder than for those with a disorder in the past month. This finding suggests that even among individuals with more severe cases of common mental disorders, the premorbid level of employment can be regained during times of remission.
Because unemployment may trigger processes that lead to the development or reoccurrence of mental disorders, persons who experienced problems retaining their jobs or returning to work may have been overrepresented in our sample group with a past-month disorder and underrepresented in our groups with a past-year and a lifetime disorder. However, even though causality may operate in both directions, in our opinion the analysis of the reasons provided for unemployment favors one direction of causality, namely from mental illness to unemployment. This is borne out by our analysis of respondents' reasons for being unemployed in the past month ( Table 5 ), which found that those with a current or past mental disorder attributed their unemployment to mental health problems or to a combination of mental health problems and general medical problems. If unemployment triggered mental health problems among survey respondents, one would not have expected the analysis to yield these results. Compared with unemployed respondents with no mental disorder, those with a past-month disorder were 17 times more likely to attribute being unemployed to their mental health problems, five times more likely to attribute it to a combination of mental health and general medical problems, and .3 times less likely to report that no health problems restricted their employment.
Analysis of reasons for unemployment also showed that respondents with a past-year or lifetime disorder were more likely to attribute their current unemployment to mental health problems than were unemployed respondents with no disorder, even though they did not have a current disorder. Why would respondents who have recovered from a mood or anxiety disorder or who were in remission cite mental health problems as the reason for being unemployed? One possibility is that they are not referring to their mental health but to the lingering stigma related to employing individuals who have had mental health problems.
Salary level was examined only among those who reported work in the previous month. As expected, earning an above-average salary was related to gender, education, and level of occupation. However, it was also related to age at onset of the disorder. That is, those who experienced a first episode of a mood or anxiety disorder before the age of 25 had lower odds of being in the above-average salary category even after the analysis adjusted for years of education and occupation. This finding replicates results of previous studies in which earlier onset of a mental disorder was related to greater impairments in psychosocial functioning ( 28 ) and to truncated education ( 29 , 30 ).
Limitations and strengths of the Israel National Health Survey have been discussed elsewhere ( 17 ). Levels of employment among persons aged 15 and older in the survey were compared with official statistics for the general population in Israel and found to be a bit higher, but the difference could be explained by the age range in the survey sample and the fact that the survey sample was a noninstitutionalized community sample ( 31 ). There is a possibility of selection bias; if individuals with mental health problems were less likely to participate, the survey would have underestimated the level of unemployment for this group. On the other hand, the survey gathered data only on mood and anxiety disorders. As a result, the group with no disorders may have included respondents with more serious mental disorders, such as schizophrenia. However, because the proportion of persons with serious mental illness in the general population is so small, the presence of these individuals in the group with no disorders would have had had little or no effect on our results.
The main limitation of the study is its cross-sectional nature. The assumption that persons with a history of a mood or anxiety disorder have recovered from a state similar to those with a current disorder is essential to the interpretation that a premorbid level of employment can be regained. However, this assumption was found to be wrong in a study of persons with past or current mental disorders—those who were working differed in many other aspects from those who did not work ( 32 ).
The cross-sectional nature of the survey is also the reason for the inability, noted above, to clearly assert that mental disorders were the cause of unemployment among respondents and not the result of it. However, even if such assumptions have sometimes proven to be incorrect, the findings of this study show that in a representative sample of the adult population of Israel, 74%–77% of respondents aged 35 to 49 who had a past but not a current mood or anxiety disorder were employed. Moreover, when they were unemployed, they were less inclined to attribute their unemployment to mental health problems. One might conclude that in community settings, where there may be a wider range of severity levels, a history of depression or anxiety does not necessitate future unemployment or even restriction to low-paying jobs. The stigma of a past mental disorder is the more likely obstacle for reemployment.
Conclusions
The study confirmed previous findings of lower employment rates among persons in the acute phase of a common mental disorder, but it also showed that employment among persons who recover from an episode of a mood or anxiety disorder can return to a rate similar to that among persons who have never had a disorder. Analysis of the reasons for unemployment led us to conclude that mental health problems were the cause of unemployment rather than the result and that the stigma related to a past mental disorder is a likely obstacle for reemployment.
Acknowledgments and disclosures
The Israel National Health Survey was carried out in conjunction with the WHO-WMH Survey Initiative and funded by the Israel Ministry of Health with additional support from the Israel National Institute for Health Policy and Health Services Research and the Israel National Insurance Institute. The authors thank the staff of the WMH Data Collection and Data Analysis Coordination Centers for assistance with instrumentation and fieldwork and consultation on data analysis. The activities of these centers were supported by grant R01-MH070884 from the National Institute of Mental Health; the John D. and Catherine T. MacArthur Foundation; the Pfizer Foundation; grants R13-MH066849, R01-MH069864, and R01-DA016558 from the U.S. Public Health Service; grant FIRCA-R03-TW006481 from the Fogarty International Center; the Pan American Health Organization; Eli Lilly and Company, Ortho-McNeil-Janssen Pharmaceuticals; GlaxoSmithKline; and Bristol-Myers Squibb. The views and opinions expressed are those of the authors and should not be construed to represent the views of any of the sponsoring organizations or of the government.
The authors report no competing interests.
1. Kessler RC, Frank RG: The impact of psychiatric disorders on work loss days. Psychological Medicine 27:861–873, 1997Google Scholar
2. Marcotte DE, Wilcox-Gök V, Redmon PD: Prevalence and patterns of major depressive disorder in the United States labor force. Journal of Mental Health Policy and Economics 2:123–131, 1999Google Scholar
3. Dewa CS, Lin E: Chronic physical illness, psychiatric disorder and disability in the workplace. Social Science and Medicine 51: 41–50, 2000Google Scholar
4. Lim D, Sanderson K, Andrews G: Lost productivity among full-time workers with mental disorders. Journal of Mental Health Policy and Economics 3:139–146, 2000Google Scholar
5. Laitinen-Krispijn S, Bijl RV: Mental disorders and employee sickness absence: the NEMESIS study. Social Psychiatry and Psychiatric Epidemiology 35:71–77, 2000Google Scholar
6. Blackmore ER, Stansfeld SA, Weller I, et al: Major depressive episodes and work stress: results from a national population survey. American Journal of Public Health 97: 2088–2093, 2007Google Scholar
7. Lerner D, Adler DA, Chang H, et al: Unemployment, job retention, and productivity loss among employees with depression. Psychiatric Services 55:1371–1378, 2004Google Scholar
8. Löwe B, Willand L, Eich W, et al: Psychiatric comorbidity and work disability in patients with inflammatory rheumatic diseases. Psychosomatic Medicine 66: 395–402, 2004Google Scholar
9. Stang PE, Brandenburg NA, Lane MC, et al: Mental and physical comorbid conditions and days in role among persons with arthritis. Psychosomatic Medicine 68:152–158, 2006Google Scholar
10. Adler DA, McLaughlin TJ, Rogers WH, et al: Job performance deficits due to depression. American Journal of Psychiatry 163: 1569–1576, 2006Google Scholar
11. Schmitz N, Wang J, Malla A, et al: Joint effect of depression and chronic conditions on disability: results from a population-based study. Psychosomatic Medicine 69:332–338, 2007Google Scholar
12. Esposito E, Wang JL, Williams JV, et al: Mood and anxiety disorders: the association with presenteeism in employed members of a general population sample. Epidemiologia e Psichiatria Sociale 16:231–237, 2007Google Scholar
13. El-Guebaly N, Currie S, Williams J, et al: Association of mood, anxiety, and substance use disorders with occupational status and disability in a community sample. Psychiatric Services 58:659–667, 2007Google Scholar
14. Chatterji P, Alegría M, Lu M, et al: Psychiatric disorders and labor market outcomes: evidence from the National Latino and Asian American Study. Health Economics 16:1069–1090, 2007Google Scholar
15. Simon GE, Chisholm D, Treglia M, et al: Course of depression, health services costs, and work productivity in an international primary care study. General Hospital Psychiatry 24:328–335, 2002Google Scholar
16. Schoenbaum M, Unützer J, McCaffrey D, et al: The effects of primary care depression treatment on patients' clinical status and employment. Health Services Research 37:1145–1158, 2002Google Scholar
17. Levinson D, Zilber N, Lerner Y, et al: Prevalence of mood and anxiety disorders: results from the Israel National Health Survey. Israel Journal of Psychiatry and Related Sciences 44:94–103, 2007Google Scholar
18. Kessler RC, Ustun TB: The World Mental Health (WMH) Survey Initiative Version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). International Journal of Methods in Psychiatric Research 13:93–121, 2004Google Scholar
19. Levinson D, Paltiel A, Nir M, et al: The Israel-World Mental Health Survey: issues and methods. Israel Journal of Psychiatry and Related Sciences 44:85–93, 2007Google Scholar
20. Haro JM, Arbabzadeh-Bouchez S, Brugha TS, et al: Concordance of the Composite International Diagnostic Interview Version 3.0 (CIDI 3.0) with standardized clinical assessments in the WHO World Mental Health Surveys. International Journal of Methods in Psychiatric Research 15:167–180, 2006Google Scholar
21. Knight M, Stewart-Brown S, Fletcher L: Estimating health needs: the impact of a checklist of conditions and quality of life measurements on health information derived from community surveys. Journal of Public Health Medicine 23:179–186, 2001Google Scholar
22. Fan VS, Au D, Heagerty P, et al: Validation of case-mix measures derived from self-reports of diagnoses and health. Journal of Clinical Epidemiology 55:371–380, 2002Google Scholar
23. Evaluation of National Health Interview Survey Diagnostic Reporting. Vital and Health Statistics, Series 2. Atlanta, Centers for Disease Control and Prevention, National Center for Health Statistics, 1994Google Scholar
24. International Standard Classification of Occupations. Geneva, International Labour Organization, 2007. Available at www.ilo.org/public/english/bureau/stat/isco/intro3.htm Google Scholar
25. SUDAAN, Version 8.0.2. Research Triangle Park, NC, Research Triangle Institute, 2003Google Scholar
26. Sanderson K, Andrews G: Common mental disorders in the workforce: recent findings from descriptive and social epidemiology Review. Canadian Journal of Psychiatry 51:63–75, 2006Google Scholar
27. Levinson D, Lerner Y, Zilber N, et al: Twelve-month service utilization rates for mental health reasons: data from the Israel National Health Survey. Israel Journal of Psychiatry and Related Sciences 44:114–125, 2007Google Scholar
28. Zisook S, Rush AJ, Albala A, et al: Factors that differentiate early vs later onset of major depression disorder. Psychiatry Research 129:127–140, 2004Google Scholar
29. Kessler RC, Foster CL, Saunders WB, et al: Social consequences of psychiatric disorders: I. educational attainment. American Journal of Psychiatry 152:1026–1032, 1995Google Scholar
30. Isohanni I, Jones PB, Järvelin MR, et al: Educational consequences of mental disorders treated in hospital: a 31-year follow-up of the Northern Finland 1966 birth cohort. Psychological Medicine 31:339–349, 2001Google Scholar
31. Levinson D, Lerner Y, Zilber N, et al: The prevalence of mental disorders and service use in Israel: results from the National Health Survey, 2003–2004, in The WHO World Mental Health Surveys: Global Perspectives on the Epidemiology of Mental Disorders. Edited by Kessler RC, Ustun TB. New York, Cambridge University Press, New York, 2008Google Scholar
32. Elinson L, Houck P, Marcus SC, et al: Depression and the ability to work. Psychiatric Services 55:29–34, 2004Google Scholar

